
SIADH for USMLE Step 3
Start your One-Week Free Trial
Already subscribed? Log in »
Syndrome of Inappropriate Antidiuretic Hormone (SIADH) for the USMLE Step 3 Exam
- Pathophysiology
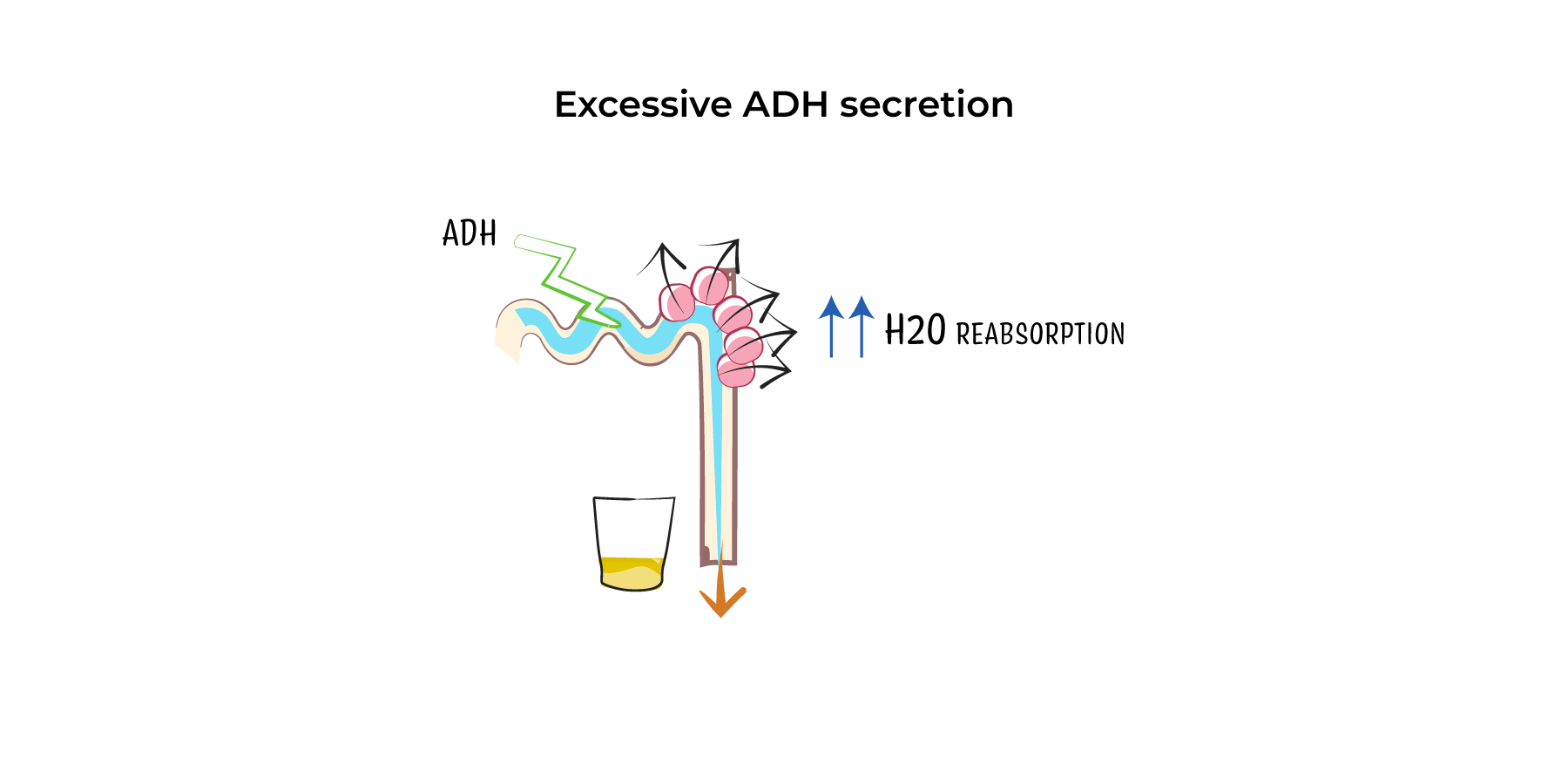
- Increased ADH Secretion: In SIADH, antidiuretic hormone (ADH) is secreted inappropriately, leading to water reabsorption by the kidneys even when plasma osmolality is low.
- Hyponatremia and Low Plasma Osmolality: Retained free water dilutes the plasma, resulting in hyponatremia and low plasma osmolality. However, urine remains inappropriately concentrated due to continued ADH action.
- No Edema: Despite water retention, there is no edema or hypervolemia because sodium levels remain normal, preventing extracellular fluid overload.
- Etiology
- CNS Disorders: Stroke, head trauma, meningitis, encephalitis, and subarachnoid hemorrhage can cause SIADH by disrupting hypothalamic regulation of ADH.
- Pulmonary Disorders: Conditions like pneumonia, tuberculosis, and chronic obstructive pulmonary disease (COPD) can stimulate ADH release.
- Malignancies: The most notable cause is small-cell lung carcinoma, which can produce ectopic ADH. Other cancers such as pancreatic or prostate cancer can also trigger SIADH.
- Medications:
- SSRIs (e.g., sertraline, fluoxetine), tricyclic antidepressants (e.g., amitriptyline).
- Anticonvulsants (e.g., carbamazepine), antipsychotics (e.g., haloperidol).
- Chemotherapy Agents (e.g., vincristine, cyclophosphamide).
- Surgery: SIADH can occur after major surgeries, often due to stress-induced ADH release.
- Clinical Features
- Mild Hyponatremia (Na+ 130–135 mEq/L): Patients may be asymptomatic or experience nonspecific symptoms like fatigue, headache, or nausea.
- Moderate Hyponatremia (Na+ 120–129 mEq/L): Symptoms may include confusion, lethargy, muscle cramps, and irritability.
- Severe Hyponatremia (Na+ <120 mEq/L): Neurological symptoms such as seizures, altered mental status, and coma due to cerebral edema from fluid shifts.
- Diagnosis
- Serum Sodium <135 mEq/L: Hyponatremia is the hallmark of SIADH.
- Low Plasma Osmolality (<275 mOsm/kg): Indicates free water retention and dilution of serum solutes.
- High Urine Osmolality (>100 mOsm/kg): Despite hyponatremia and low plasma osmolality, urine remains concentrated due to ADH action.
- Elevated Urine Sodium (>20–30 mEq/L): Reflects ongoing renal sodium excretion despite hyponatremia.
- Normal Thyroid, Adrenal, and Renal Function: These must be normal to rule out other causes of hyponatremia (e.g., hypothyroidism, adrenal insufficiency).
- Management
- Fluid Restriction:
- First-line treatment for most cases, restricting fluid intake to 500–1,000 mL/day to reduce water retention.
- Hypertonic Saline (3%):
- Used for severe or symptomatic hyponatremia (e.g., seizures, coma). Sodium correction should be slow (no more than 4–6 mEq/L in 24 hours) to avoid osmotic demyelination syndrome (ODS).
- Medications:
- Vasopressin Receptor Antagonists (Vaptans): Tolvaptan or conivaptan blocks ADH at the V2 receptor, leading to increased free water excretion.
- Demeclocycline: Causes nephrogenic diabetes insipidus, reducing water reabsorption, but is typically reserved for chronic cases due to potential nephrotoxicity.
- Loop Diuretics: Furosemide can be used to increase free water excretion while minimizing sodium loss, especially in conjunction with oral salt supplementation.
- Complications
- Severe Hyponatremia: Can result in seizures, coma, and even death if untreated.
- Osmotic Demyelination Syndrome (ODS): Rapid correction of sodium levels can cause demyelination in the brainstem, leading to irreversible neurological damage, including quadriplegia, dysphagia, and altered consciousness.
Key Points
- Pathophysiology: SIADH is characterized by excessive ADH secretion, leading to free water retention, dilutional hyponatremia, and concentrated urine.
- Causes: Common triggers include CNS disorders, lung diseases, small-cell lung cancer, medications (e.g., SSRIs, anticonvulsants), and postoperative states.
- Symptoms: Mild cases may be asymptomatic, while severe hyponatremia can cause confusion, seizures, or coma.
- Diagnosis: Identified by hyponatremia, low plasma osmolality, high urine osmolality, and normal thyroid, adrenal, and renal function.
- Treatment: Fluid restriction is the cornerstone of therapy; hypertonic saline for severe cases; and vasopressin antagonists or demeclocycline for chronic SIADH.
- Complications: Rapid correction of hyponatremia can lead to osmotic demyelination syndrome, causing permanent neurological damage.