
USMLE/COMLEX 3 - Malabsorption Syndromes
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for USMLE Step 3 & COMLEX-USA Level 3 from the Malabsorption Syndromes tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
 Below is information not explicitly contained within the tutorial but important for USMLE & COMLEX 3.
Below is information not explicitly contained within the tutorial but important for USMLE & COMLEX 3.
- --
VITAL FOR USMLE/COMLEX 3
Diagnostic Approach to Malabsorption
1. Malabsorption is failure to assimilate nutrients due to defects in digestion, absorption, or transport resulting from deficient digestive agents, abnormal GI epithelium, impaired transport, short bowel, or inadequate mixing.
2. Key symptoms include diarrhea, steatorrhea, weight loss, weakness, anemia, and vitamin/mineral deficiencies that can lead to musculoskeletal, neurologic, and cardiac complications.
3. Diagnosis requires patient history (stool type & frequencies, weight loss), blood tests for specific nutrient deficiencies, fecal fat tests and Sudan III staining, with further investigation using endoscopy, colonoscopy with biopsy, breath tests, or small bowel imaging.
4. Management focuses on treating the underlying cause while addressing nutritional deficiencies.
Exocrine Pancreatic Insufficiency (EPI)
1. Occurs when over A90% of pancreatic enzyme function is lost, primarily affecting fat and fat-soluble vitamin absorption (A, D, E, K, B12).
2. Major etiologies include pancreatitis (often alcohol-related in adults), cystic fibrosis (most common pediatric cause), and tumors obstructing pancreatic ducts.
3. Diagnosis relies on reduced duodenal pH and fecal elastase-1 (FE-1) levels.
4. Clinical features include loose, bulky, oily, pale stools that often float, and pancreatitis patients experience left epigastric pain radiating to the back.
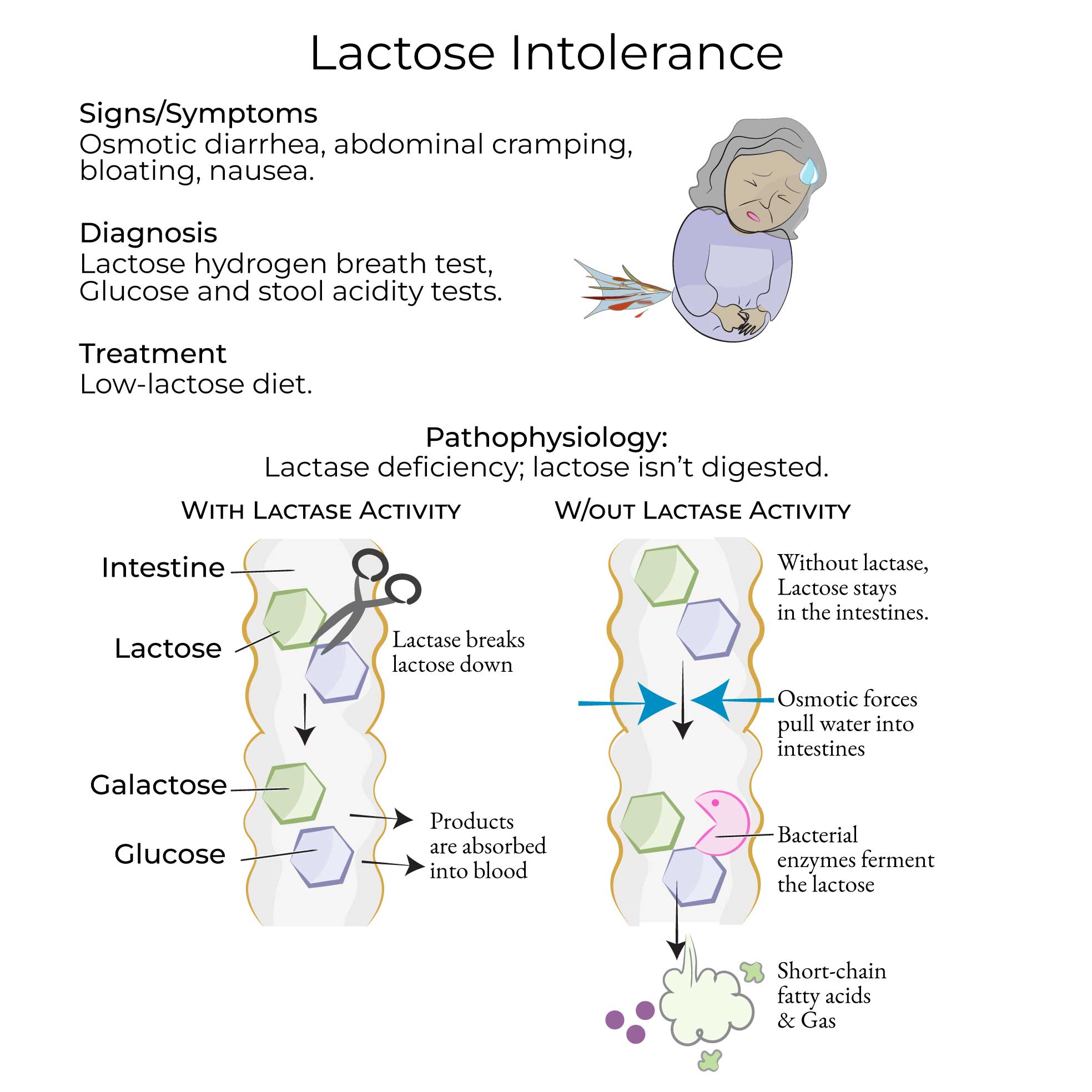
Lactose Intolerance
1. Results from deficient lactase activity with high prevalence (>65% worldwide) varying by population (30% Europe, 50% US, 70% Asia, nearly 100% Africa).
2. Types include congenital (rare autosomal recessive), primary (common adult-type), and secondary (transient due to intestinal damage).
3. Pathophysiology involves osmotic diarrhea from undigested lactose and gas/pain from bacterial fermentation.
4. Diagnosis uses hydrogen breath test (>20 ppm increase indicates deficiency), blood glucose tests, DNA tests, and stool acidity tests.
Celiac Disease
1. Autoimmune inflammatory disorder affecting 1% of US adults, triggered by gliadin in wheat, barley, and rye.
2. Diagnosis requires serological screening (tTG-IgA, tTG-IgG, deamidated gliadin peptide antibodies, EMA-IgA) followed by endoscopy with small bowel biopsy.
3. Histopathology shows increased lymphocytes, mucosal inflammation, villous atrophy, and crypt hyperplasia with endoscopic findings of duodenal scalloping and hypervascularity.
4. Associated conditions include dermatitis herpetiformis (10% of patients), reduced bone density, and increased malignancy risk.
Whipple Disease
1. Rare bacterial infection caused by Tropheryma whipplei, primarily affecting older males of European descent with immune defects.
2. Clinical course begins with arthralgias, followed by neurologic symptoms (dementia), endocarditis, and later GI effects (diarrhea, abdominal pain, weight loss).
3. Diagnosis requires small bowel biopsy with PAS-positive staining showing foamy macrophages in lamina propria and villous atrophy.
4. PCR testing for T. whipplei DNA in CSF is essential due to neurologic complications.
- --
HIGH YIELD
Treatment Strategies
1. EPI: Management includes lifestyle modifications (alcohol cessation), vitamin supplements, and exogenous pancreatic enzyme administration.
2. Lactose Intolerance: Patients should reduce consumption of lactose-rich foods based on individual tolerance levels.
3. Celiac Disease: Strict gluten-free diet is the only effective treatment.
4. Tropical Sprue: Therapy combines folic acid and Vitamin B12 supplementation with antibiotics (tetracycline, ampicillin).
5. Whipple Disease: Antibiotic regimen of ceftriaxone or penicillin followed by trimethoprim/sulfamethoxazole; fatal without treatment and relapses are common.
Diagnostic Pearls
1. EPI affects primarily fat digestion because carbohydrate and protein digestion are maintained by enzymes from salivary glands, stomach, and small intestine.
2. Primary vs secondary lactase deficiency: intestinal villi appear normal in primary but damaged in secondary cases.
3. Lactose intolerance differs from milk allergy, which is an immune-mediated reaction to cow's milk proteins.
4. Celiac disease and tropical sprue have similar histopathology, requiring serologic tests for differentiation.
5. HLA-DQ2 and HLA-DQ8 haplotypes are common in the general population, making them mainly useful for ruling out celiac disease when negative.
Clinical Management Challenges
1. Chronic pancreatitis can lead to both endocrine and exocrine pancreatic insufficiency, resulting in diabetes mellitus alongside malabsorption.
2. Secondary lactase deficiency is a transient condition that may resolve when underlying intestinal damage heals.
3. Whipple disease neurologic complications can be disabling, necessitating CSF testing and aggressive treatment.
4. Untreated celiac disease increases risk for complications including malignancy and bone disease.
5. Tropical sprue diagnosis requires ruling out celiac disease through serologic testing due to similar histopathologic findings.
- --
Beyond the Tutorial
Advanced Management Considerations
1. Monitoring therapeutic response: Evidence-based protocols for following patients on treatment.
2. Managing refractory cases: Systematic approach when first-line therapies fail.
3. Parenteral nutrition indications: When to initiate alternative feeding methods.
4. Multidisciplinary team approach: Coordination between gastroenterology, nutrition, and other specialties.
5. Telehealth strategies: Remote monitoring of patients with chronic malabsorption disorders.
Clinical Decision Making
1. Diagnostic algorithms: Cost-effective approaches to the patient with suspected malabsorption.
2. Risk stratification: Identifying patients who need urgent intervention versus outpatient workup.
3. Treatment selection: Personalized therapies based on disease severity and comorbidities.
4. Prevention strategies: Reducing complications in high-risk populations.
5. Chronic disease management: Long-term follow-up protocols and monitoring parameters.
Complex Patient Scenarios
1. Malabsorption in pregnancy: Management modifications and fetal considerations.
2. Elderly patients: Altered presentation and treatment adaptations.
3. Medication absorption issues: Adjusting drug regimens in malabsorptive states.
4. Post-surgical patients: Approach to iatrogenic malabsorption following GI surgeries.
5. Patients with multiple GI disorders: Managing overlapping conditions affecting absorption.