
USMLE/COMLEX 2 - Medium & Variable Vessel Vasculitis
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for USMLE Step 2 & COMLEX-USA Level 2 from the Medium & Variable Size Vessel Vasculitis tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
- --
VITAL FOR USMLE/COMLEX 2
General Concepts of Vasculitis
1. Vasculitides cause blood vessel inflammation, leading to ischemia, necrosis, and organ damage.
2. General systemic signs include fever, weight loss, fatigue, arthralgias, myalgias.
3. First-line treatment for most vasculitides is high-dose corticosteroids to prevent permanent end-organ damage.
Polyarteritis Nodosa (PAN)
4. PAN is a medium-sized muscular artery necrotizing vasculitis.
5. Multisystem involvement is typical:
- Peripheral nervous system: mononeuritis multiplex (asymmetric neuropathy affecting median, ulnar, fibular nerves)
- Renal: hypertension, renal insufficiency (without glomerulonephritis)
- GI: abdominal pain, mesenteric ischemia, risk of aneurysm rupture
- Skin: livedo reticularis, ulcers, nodules, gangrene
- Heart: coronary artery ischemia and heart failure
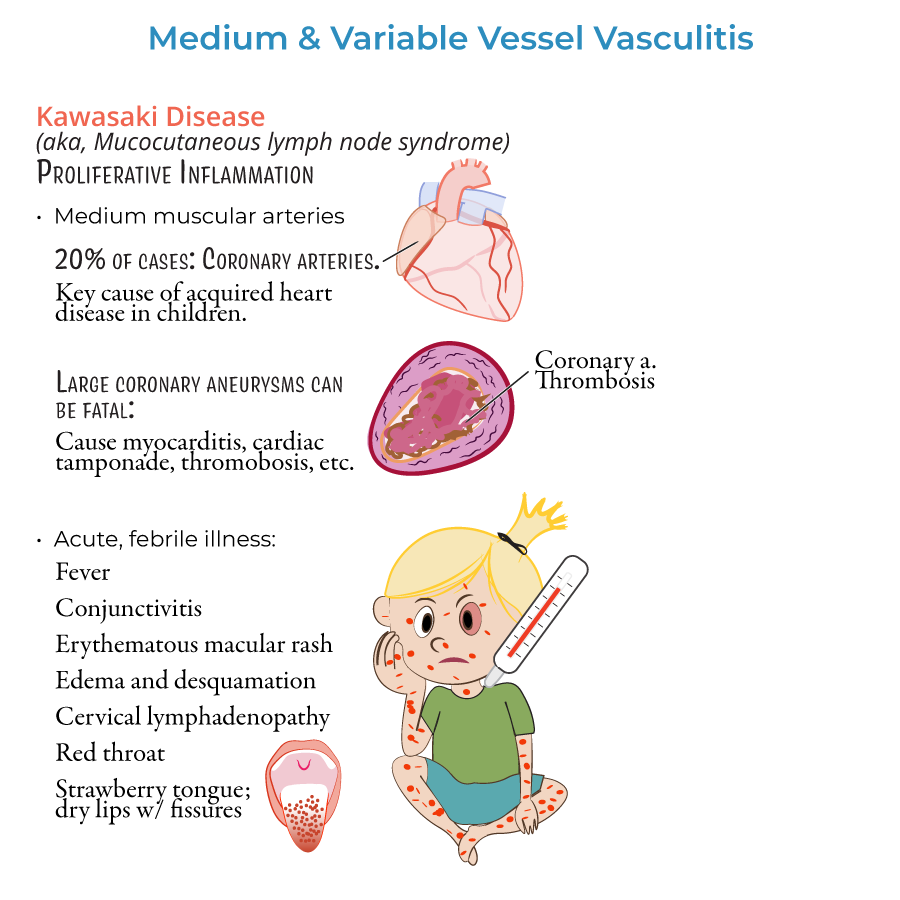
Kawasaki Disease
9. Kawasaki disease is a medium-vessel vasculitis primarily affecting young children (<5 years).
10. Diagnostic criteria:
- Fever ≥5 days and at least 4 of the following:
- Bilateral conjunctival injection
- Oral mucous membrane changes (strawberry tongue, fissured lips)
- Polymorphous rash
- Extremity changes (edema, desquamation)
- Cervical lymphadenopathy (>1.5 cm node)
- --
HIGH YIELD
Behçet Disease
1. Behçet disease affects vessels of all sizes.
2. Clinical presentation includes:
- Recurrent oral and genital ulcers
- Ocular inflammation (anterior or posterior uveitis, hypopyon)
- Skin lesions (erythema nodosum, papulopustular lesions)
- Arthritis and possible vascular thrombosis
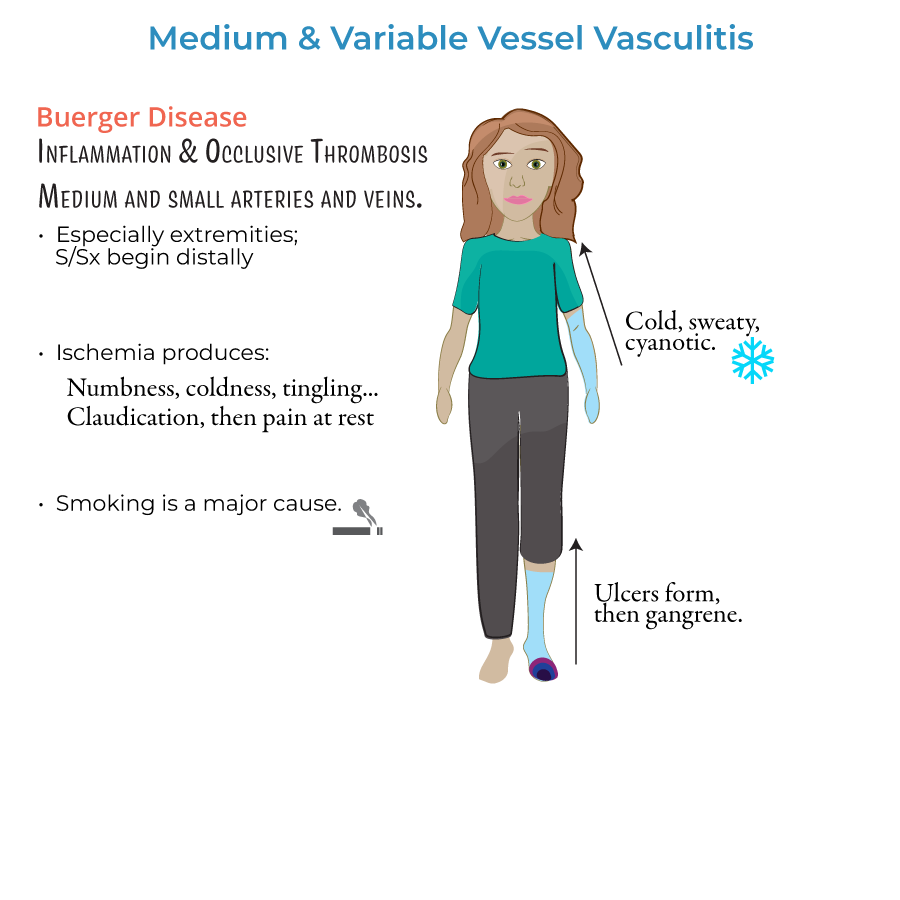
Buerger Disease (Thromboangiitis Obliterans)
6. Buerger disease involves small- and medium-sized vessels, typically in young male smokers.
7. Symptoms:
- Distal ischemia (cold, numbness, claudication)
- Ulcers, gangrene
- Superficial thrombophlebitis
Histology and Additional Diagnostic Points
10. PAN histology: transmural necrotizing inflammation of medium arteries.
11. Kawasaki histology: proliferative arteritis, especially coronary arteries.
12. Behçet: neutrophilic vasculitis on biopsy.
13. Buerger disease: thrombosis and inflammation sparing the vessel wall.
- --
Beyond the Tutorial
PAN-Specific Notes
1. Negative ANCA testing distinguishes PAN from ANCA-associated vasculitides.
2. PAN commonly spares the lungs, which helps differentiate it from GPA (Granulomatosis with polyangiitis).
Kawasaki Disease Follow-Up
3. Repeat echocardiogram at 2 and 6 weeks after initial diagnosis to monitor for evolving coronary aneurysms.
4. Risk of thrombosis and myocardial infarction persists in the presence of coronary aneurysms despite treatment.
Behçet Disease Monitoring
5. Monitor for eye complications — untreated ocular involvement can lead to blindness.
6. Risk of deep vein thrombosis (DVT) is increased in Behçet’s due to vascular inflammation.
Buerger Disease Clinical Integration
7. Often coexists with Raynaud phenomenon.
8. No role for anticoagulation unless thrombosis of large vessels is present.