
USMLE/COMLEX 2 - Large Vessel Vasculitis
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for USMLE Step 2 & COMLEX-USA Level 2 from the Large Vessel Vasculitis tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
- --
VITAL FOR USMLE/COMLEX 2
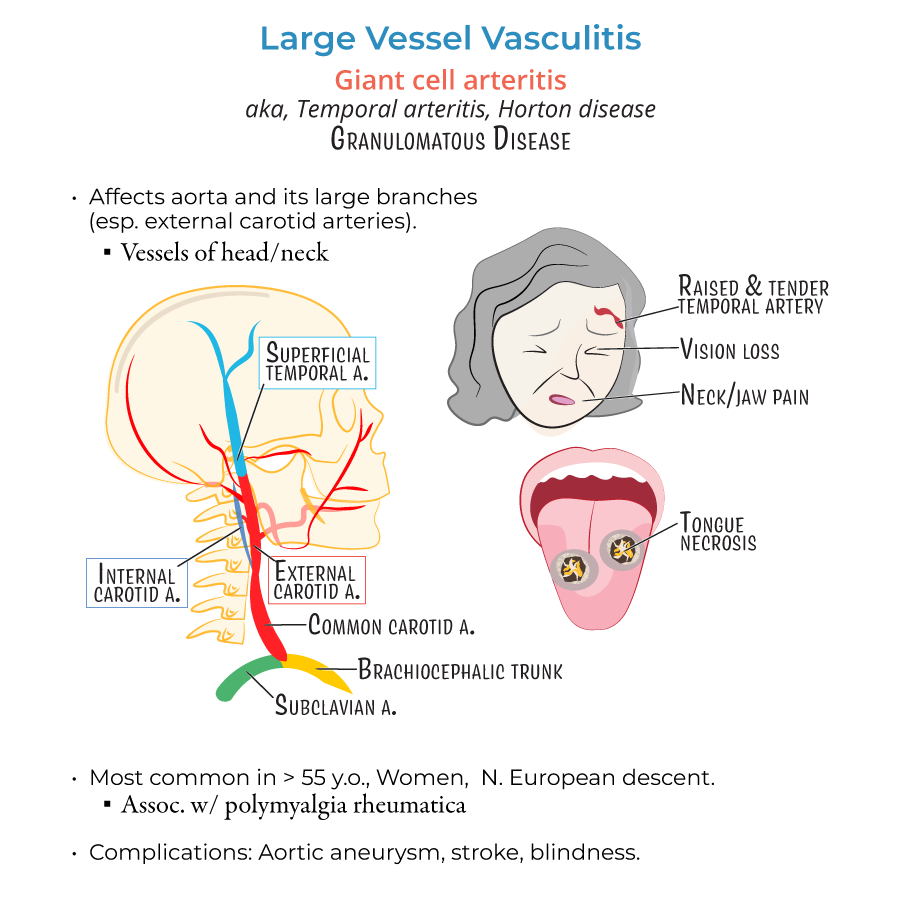
Clinical Features and Diagnosis of Giant Cell Arteritis (GCA)
1. GCA affects women over 50, especially of Northern European descent, and is associated with polymyalgia rheumatica in up to 50% of cases.
2. Classic symptoms include:
- New-onset temporal headache
- Jaw claudication
- Scalp tenderness
- Visual disturbances, especially amaurosis fugax (transient monocular blindness)
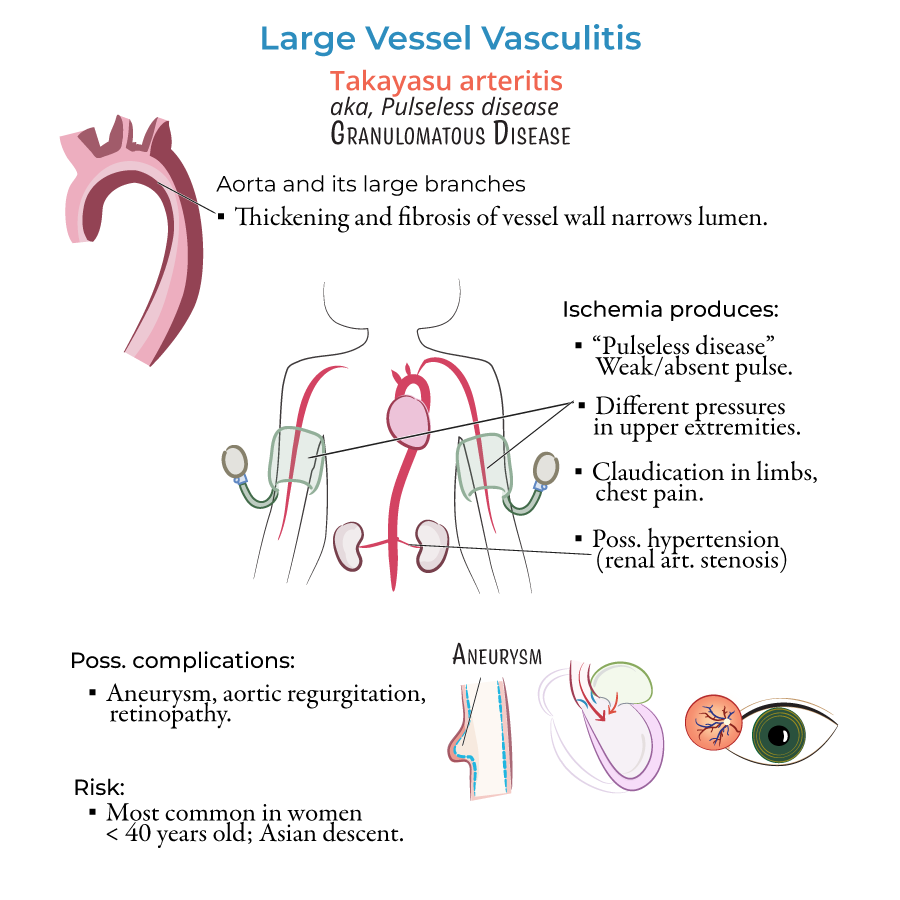
Clinical Features and Diagnosis of Takayasu Arteritis
7. Most commonly affects young women <40, especially of Asian descent.
8. Presents with:
- Decreased or absent pulses
- Blood pressure discrepancy between arms
- Limb claudication
- Carotid or subclavian bruits
- Hypertension from renal artery involvement
- --
HIGH YIELD
Disease Mechanism and Pathology
1. Both GCA and Takayasu are granulomatous vasculitides of large vessels, affecting the aorta and its major branches.
2. In GCA, inflammation targets branches of the external carotid artery, especially the temporal artery.
3. In Takayasu, inflammation affects the aortic arch and its branches, leading to stenosis and ischemia.
4. Histologically, GCA shows:
- Granulomatous inflammation
- Multinucleated giant cells
- Destruction of the internal elastic lamina
- Intimal hyperplasia
Associated Conditions and Risks
6. Polymyalgia rheumatica presents with proximal muscle pain and stiffness, elevated ESR, and rapid response to low-dose steroids.
7. GCA is a major cause of permanent vision loss in the elderly if untreated.
8. Complications of Takayasu include:
- Aortic aneurysm
- Aortic regurgitation
- Renal artery stenosis leading to hypertension
- Retinopathy
Clinical Evaluation and Management Nuances
9. Temporal artery biopsy may yield false negatives due to segmental involvement, so clinical diagnosis may supersede pathology.
10. Imaging (CT/MRI) is preferred for Takayasu, not temporal biopsy.
11. Monitor treatment response with ESR/CRP trends.
- --
Beyond the Tutorial
Decision-Making and Management Strategy
1. For suspected GCA with visual symptoms, start corticosteroids immediately, even before confirming with biopsy.
2. Methylprednisolone IV is used in severe or vision-threatening GCA cases, then transitioned to oral prednisone.
3. Steroid-sparing agents (e.g., methotrexate or tocilizumab) may be considered for patients with frequent relapses or long-term steroid complications.
4. Ophthalmology consultation is crucial for GCA patients with visual complaints.
5. Vascular surgery or rheumatology referral may be appropriate in Takayasu for severe arterial compromise.
Long-Term Follow-Up
6. Monitor for relapse, steroid side effects, and vascular complications with serial ESR/CRP and imaging.
7. Long-term steroids increase risk of osteoporosis, hyperglycemia, and infection; co-prescribe calcium, vitamin D, and consider bisphosphonates.
8. In Takayasu, BP should be measured in both arms, and renal function monitored closely.