
USMLE/COMLEX 2 - Bacterial Endocarditis
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for USMLE Step 2 CK & COMLEX-USA Level 2 from the Bacterial Endocarditis tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards.
 Below is information not explicitly contained within the tutorial but important for USMLE Step 2 CK & COMLEX-USA Level 2.
Below is information not explicitly contained within the tutorial but important for USMLE Step 2 CK & COMLEX-USA Level 2.
- --
VITAL FOR USMLE/COMLEX 2
Clinical Significance
1. Staphylococcus aureus is the leading cause of infective endocarditis; associated with a high mortality rate due to its aggressive nature and antibiotic resistance.
2. High-risk populations include individuals with compromised immune systems and/or prosthetic cardiac devices.
3. Embolic complications are common as vegetations can break free and cause embolism, even stroke.
Pathophysiology Relevant to Clinical Presentation
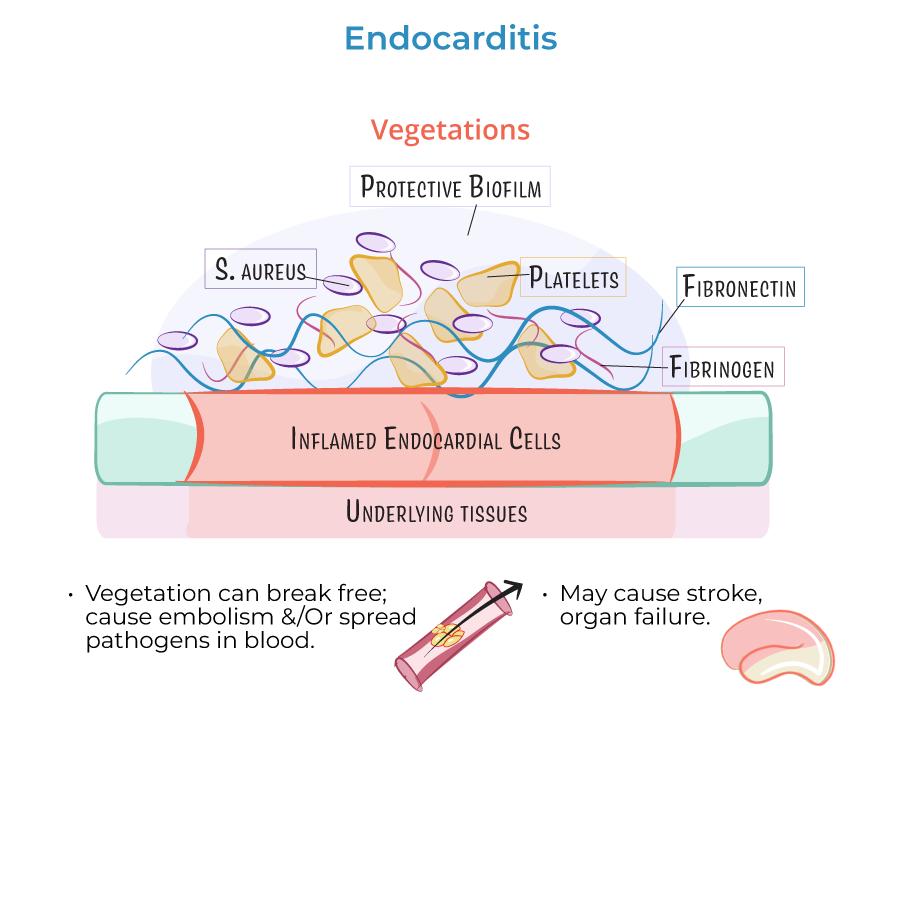
1. S. aureus produces a protective biofilm (slime layer) comprising polysaccharides and proteins that inhibit thrombus destruction, allowing proliferation and tissue destruction.
2. Within host cells, S. aureus releases toxins and acts as a superantigen to provoke immune responses that ultimately destroy the cells.
3. S. aureus can lie dormant within host tissues as small colony variants, evading host defenses and antibiotics, only to reemerge later as an infective pathogen.
Diagnostic Considerations
1. S. aureus exists in the normal human flora, commonly found in the nares (nostrils), which can be a source of bacteremia.
2. Infective endocarditis presents with vegetations on heart valves (particularly atrioventricular valve) or heart walls (mural endocarditis).
3. Vegetations are composed of fibronectin, fibrinogen, platelets, and bacteria forming thrombotic masses that can obstruct blood flow.
Treatment Approach
1. Requires prolonged intravenous administration of antibiotics; S. aureus is resistant to penicillin.
2. For methicillin-resistant strains (MRSA), vancomycin or daptomycin, sometimes in combination with other antibiotics, are administered intravenously.
3. Treatment must address both the active infection and the risk of embolic complications.
- --
HIGH YIELD
Clinical Features and Complications
1. Inflammation affects valves with vegetation blocking blood flow, which can lead to valvular dysfunction.
2. If vegetation breaks free from the valve and travels in the bloodstream, it can become lodged in a vessel and cause embolism, even stroke.
3. The aggressive nature of S. aureus causes highly destructive inflammatory processes to host tissues.
Pathogenesis Details Relevant to Management
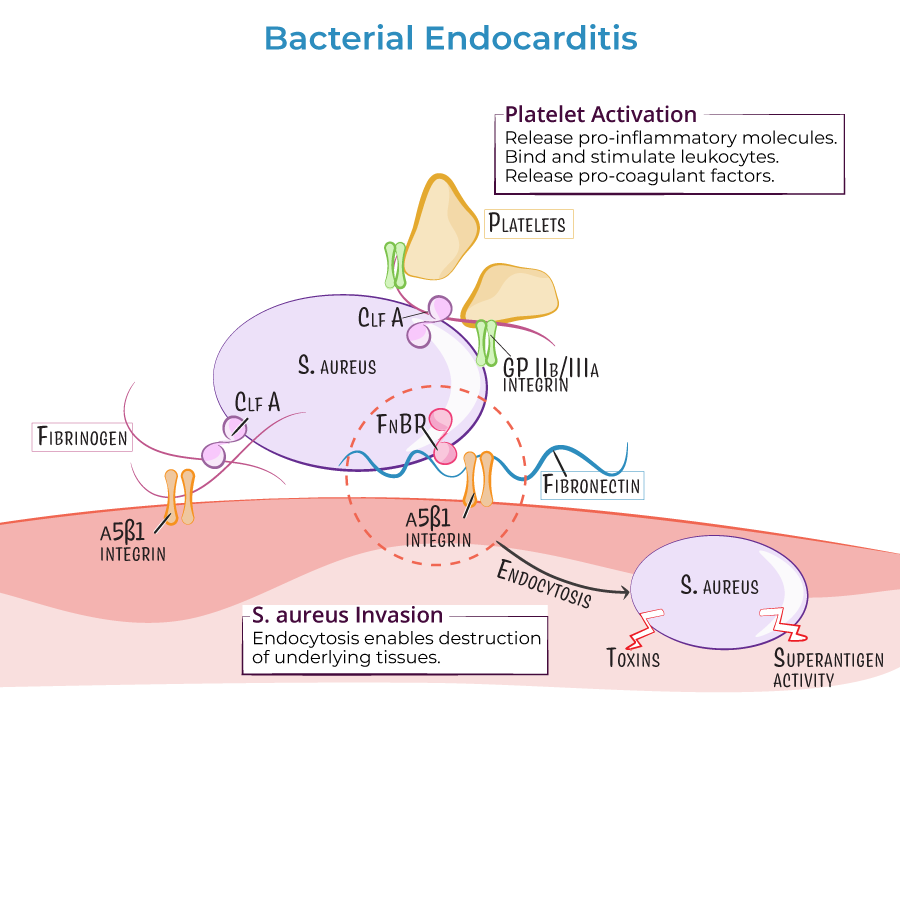
1. S. aureus adheres to endothelial cells via surface adhesion proteins, enabling colonization.
2. Invasion of endocardial cells allows bacteria to release toxins protected from immune responses.
3. Evasion of host defenses through biofilm formation and phenotype switching to small colony variants makes eradication difficult.
4. Platelet activation induces release of pro-inflammatory molecules, binding and stimulation of leukocytes, and release of pro-coagulation molecules, worsening thrombus formation.
Treatment Challenges
1. S. aureus is resistant to penicillin, limiting first-line treatment options.
2. Methicillin-resistant strains (MRSA) display changes in penicillin-binding proteins to increase tolerance.
3. MRSA is increasingly common in both hospital and community settings, requiring broader-spectrum antibiotic coverage.
4. The protective biofilm and intracellular location of bacteria can significantly reduce antibiotic effectiveness.
Risk Assessment
1. S. aureus endocarditis has a particularly high mortality rate compared to other causes of endocarditis.
2. Risk increases with compromised immune systems and/or prosthetic cardiac devices.
3. Community-acquired MRSA presents different clinical challenges than hospital-acquired strains.
- --
Beyond the Tutorial
Clinical Diagnosis and Management
1. Modified Duke criteria are essential for diagnosis, including major criteria (positive blood cultures, echocardiographic evidence) and minor criteria (predisposition, fever, vascular/immunologic phenomena).
2. Transesophageal echocardiography (TEE) is preferred over transthoracic (TTE) for detecting vegetations, especially with prosthetic valves.
3. Blood cultures should be obtained before initiating antibiotics; at least three sets from different venipuncture sites are recommended.
Treatment Guidelines
1. Empiric therapy should cover MRSA until susceptibilities are known; definitive therapy is guided by antimicrobial susceptibility testing.
2. Treatment duration typically ranges from 4-6 weeks, depending on involvement of native vs. prosthetic valves.
3. Surgical intervention is indicated for heart failure, persistent infection despite appropriate antibiotics, perivalvular extension, or large vegetations with high embolic risk.
Prevention and Follow-up
1. Antibiotic prophylaxis is recommended only for highest-risk cardiac conditions undergoing dental procedures.
2. Follow-up echocardiography is important to assess vegetation resolution and valvular function.
3. Patients who survive endocarditis require long-term cardiology follow-up for potential late complications including congestive heart failure and valvular stenosis or regurgitation.