
SIADH for USMLE Step 1
Start your One-Week Free Trial
Already subscribed? Log in »
Syndrome of Inappropriate Antidiuretic Hormone (SIADH) for the USMLE Step 1 Exam
- Pathophysiology
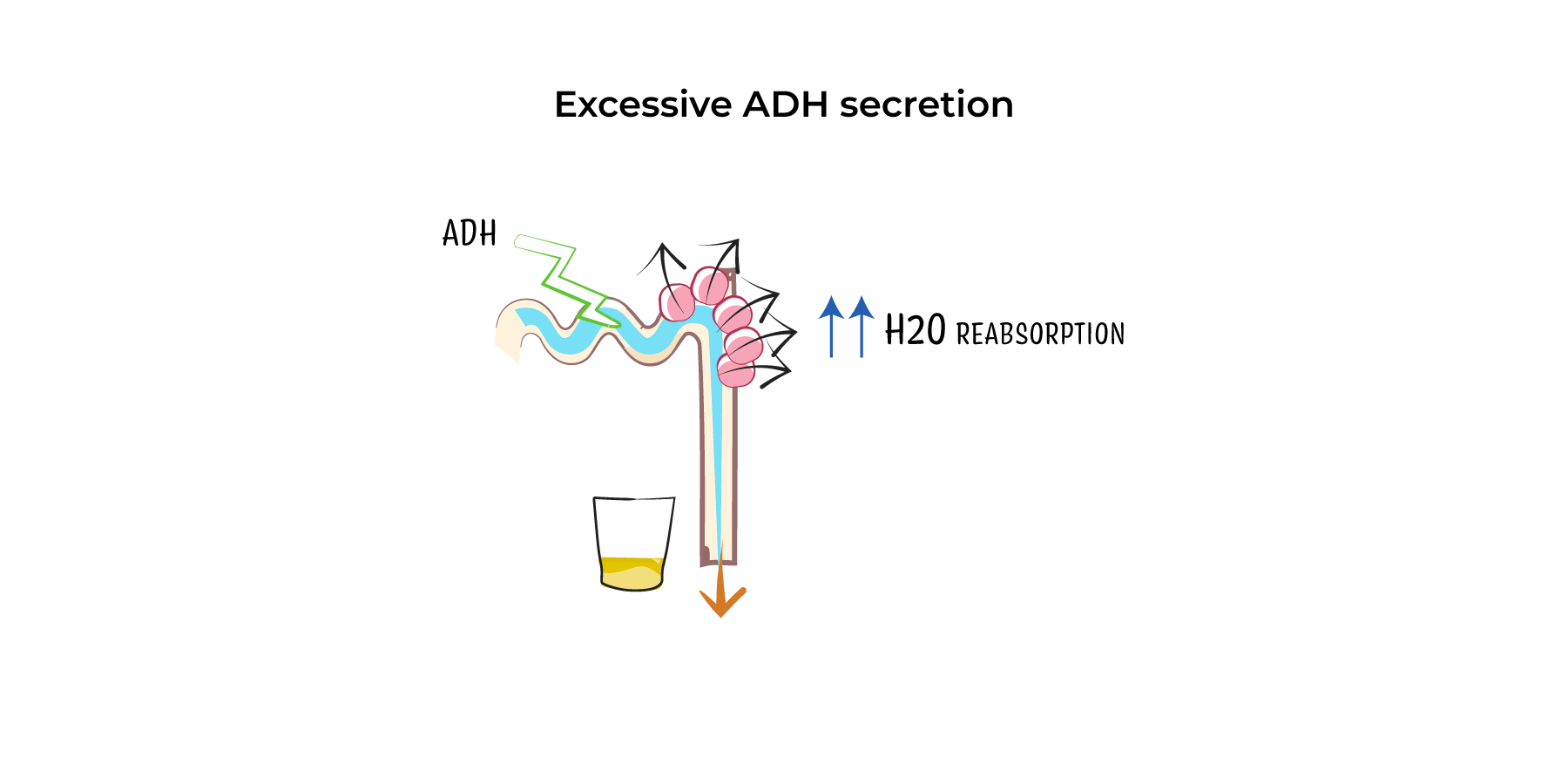
- Excess ADH Secretion: In SIADH, antidiuretic hormone (ADH) is secreted inappropriately, leading to excessive water reabsorption in the kidneys. This results in water retention and dilutional hyponatremia.
- Hyponatremia with Low Plasma Osmolality: Despite low plasma osmolality, the kidney continues to reabsorb water, concentrating the urine (high urine osmolality). However, total body sodium remains normal or slightly increased.
- No Edema: Unlike hypervolemic conditions (e.g., heart failure), SIADH causes intracellular fluid retention without peripheral edema due to normal total body sodium.
- Etiology
- Central Nervous System (CNS) Disorders: Conditions such as stroke, head trauma, meningitis, or encephalitis can disrupt ADH regulation by affecting the hypothalamus or pituitary gland.
- Pulmonary Diseases: Pneumonia, tuberculosis, or chronic obstructive pulmonary disease (COPD) can trigger SIADH due to increased ADH release.
- Malignancies: Small-cell lung carcinoma is a common malignancy associated with ectopic ADH production. Other cancers like pancreatic or prostate cancers may also cause SIADH.
- Medications: Common drugs include:
- Selective Serotonin Reuptake Inhibitors (SSRIs): Fluoxetine, sertraline.
- Antipsychotics: Haloperidol.
- Anticonvulsants: Carbamazepine.
- Chemotherapy: Cyclophosphamide and vincristine.
- Surgery: Post-operative ADH release is often seen after major surgeries.
- Clinical Features
- Mild Hyponatremia (Na+ 130–135 mEq/L): Often asymptomatic or presents with nausea, headache, or mild lethargy.
- Moderate Hyponatremia (Na+ 120–129 mEq/L): Symptoms may include confusion, dizziness, muscle cramps, and difficulty concentrating.
- Severe Hyponatremia (Na+ <120 mEq/L): Neurological symptoms like seizures, altered mental status, and even coma due to cerebral edema from fluid shifts into brain cells.
- Diagnosis
- Hyponatremia with Low Plasma Osmolality: Serum sodium <135 mEq/L with plasma osmolality <275 mOsm/kg.
- Inappropriately High Urine Osmolality: Urine osmolality >100 mOsm/kg, despite low plasma osmolality.
- Elevated Urine Sodium (>20–30 mEq/L): Demonstrates inappropriate sodium retention in the context of hyponatremia.
- Euvolemia: Clinical evaluation should show no signs of hypovolemia (e.g., dehydration, orthostatic hypotension) or hypervolemia (e.g., edema, ascites).
- Normal Adrenal, Thyroid, and Renal Function: Other causes of hyponatremia (e.g., adrenal insufficiency, hypothyroidism) must be excluded.
- Management
- Fluid Restriction: Primary treatment for mild to moderate SIADH is limiting free water intake to 500–1,000 mL/day.
- Hypertonic Saline (3%): Used for severe hyponatremia with neurologic symptoms, such as seizures or coma. Correct serum sodium slowly (increase by no more than 4–6 mEq/L in 24 hours) to avoid osmotic demyelination syndrome (ODS).
- Medications:
- Vasopressin Receptor Antagonists (Vaptans): Drugs like tolvaptan block ADH action at the renal V2 receptor, increasing free water excretion.
- Demeclocycline: An antibiotic that induces nephrogenic diabetes insipidus and is used in refractory cases.
- Oral Salt Tablets or Loop Diuretics: These may be used in chronic SIADH to promote water excretion while maintaining sodium balance.
- Complications
- Severe Hyponatremia: Can cause seizures, coma, and permanent neurologic damage if not corrected promptly.
- Osmotic Demyelination Syndrome (ODS): Overly rapid correction of hyponatremia may lead to irreversible demyelination of neurons, causing quadriplegia, dysphagia, and other neurological deficits.
Key Points
- Pathophysiology: SIADH results in excessive ADH secretion, leading to water retention, dilutional hyponatremia, and high urine osmolality without edema.
- Causes: Common causes include CNS disorders, pulmonary diseases, malignancies (especially small-cell lung cancer), medications (SSRIs, anticonvulsants), and post-surgery states.
- Symptoms: Mild hyponatremia may be asymptomatic, while severe hyponatremia can cause seizures, confusion, and coma.
- Diagnosis: Based on hyponatremia, low plasma osmolality, high urine osmolality, and euvolemia.
- Management: Treatment includes fluid restriction, hypertonic saline for severe cases, and vasopressin receptor antagonists. Avoid rapid correction to prevent osmotic demyelination syndrome.