
USMLE/COMLEX 1 - Endocarditis
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for USMLE/COMLEX 1 from the Endocarditis tutorial, as well as points of interest at the end that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
 Additional information not explicitly contained in the tutorial but important for USMLE & COMLEX 1:
Additional information not explicitly contained in the tutorial but important for USMLE & COMLEX 1:
- --
VITAL FOR USMLE/COMLEX 1
Definition and Basic Pathology
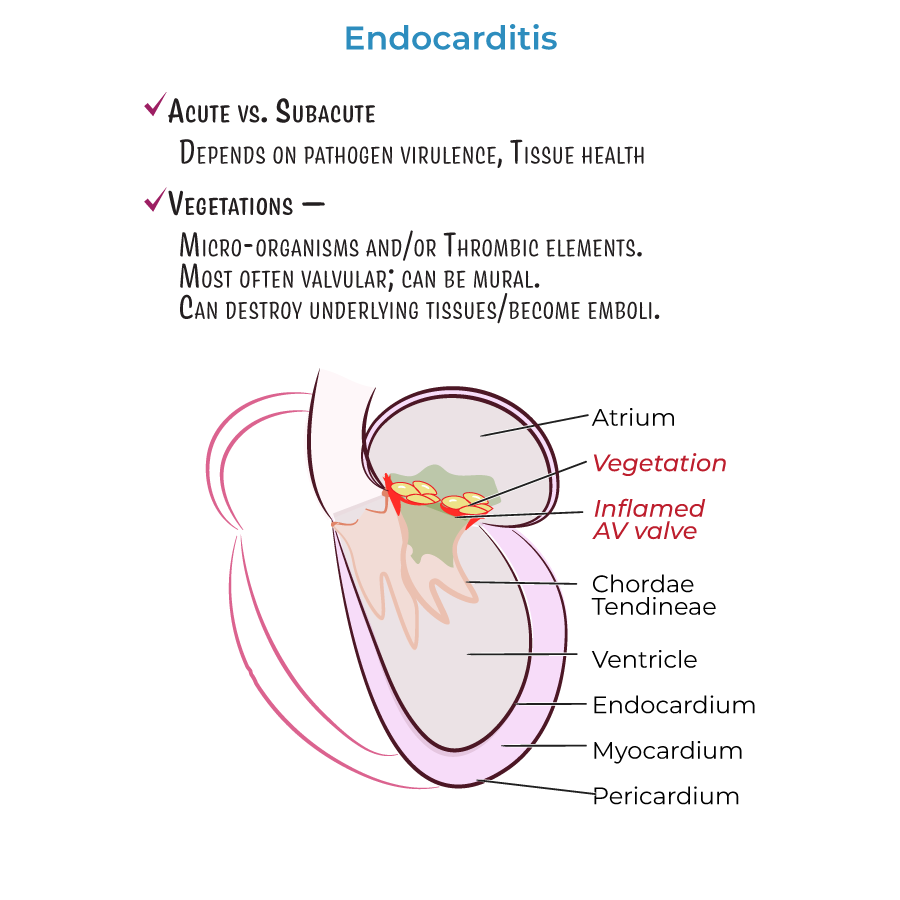
1. Endocarditis = inflammation of the internal lining of the heart (endocardium).
2. Characterized by vegetations comprising microorganisms and/or thrombotic elements.
3. Can be acute or subacute, depending on pathogen virulence and cardiac tissue health.
4. Most vegetations found on valvular ring or leaflets; "mural" vegetations form on heart walls.
5. Complications include tissue invasion/destruction and emboli formation leading to stroke, organ failure, and sepsis.
Classification of Endocarditis
1. Infective endocarditis: Contains pathogens in vegetations (also called bacterial endocarditis).
2. Non-infective endocarditis: Contains sterile vegetations (also called marantic or non-bacterial thrombotic endocarditis).
3. Culture-negative endocarditis: Infectious agent present but not identifiable by routine blood cultures.
Common Causes
1. Gram-positive bacteria most common in infective endocarditis:
- Staphylococcus aureus (most common)
- Viridans group Streptococci
- Enterococci
- Coagulase-negative Staphylococci
- Haemophilus species
- Aggregatibacter species
- Cardiobacterium hominis
- Eikenella corrodens
- Kingella kingae
- --
HIGH YIELD
Vegetation Formation
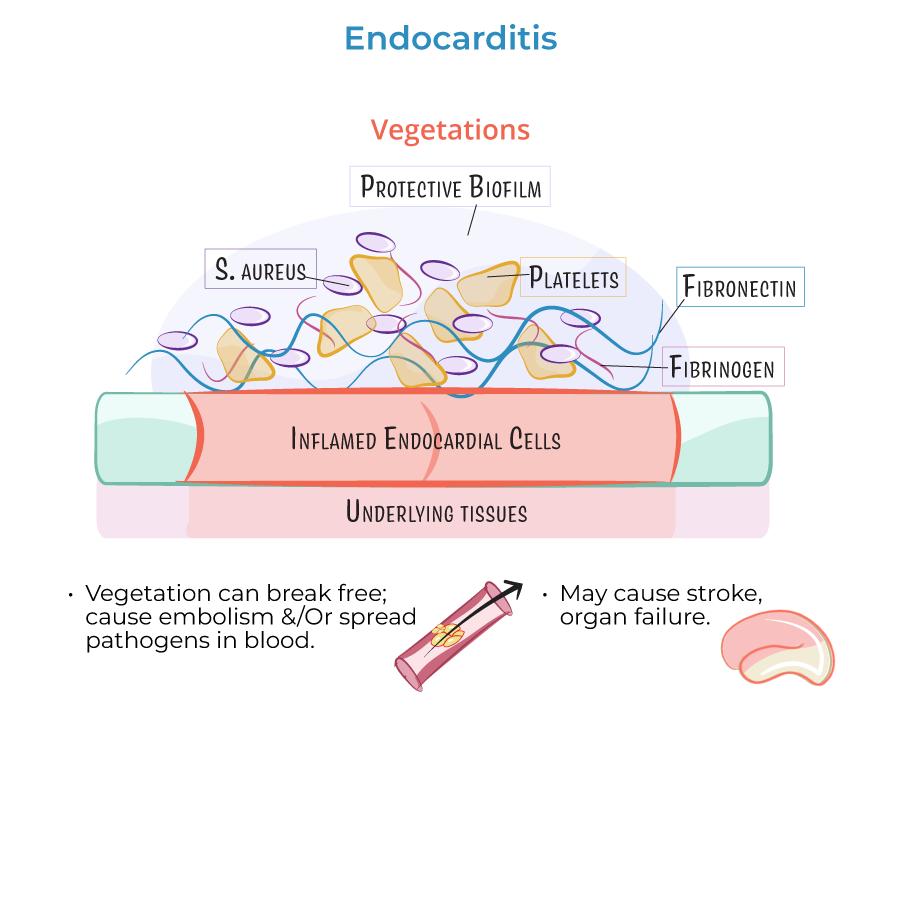
1. More likely to form where valvular damage already exists.
2. Endothelial damage promotes fibronectin deposition and vegetation formation.
3. Fibronectin adheres to circulating fibrin, platelets, white blood cells, and pathogens.
4. Vegetations can break free and cause embolism or spread pathogens systemically.
Risk Factors and Patterns
1. Turbulent blood flow promotes vegetation formation:
- Mitral valve regurgitation: Produces lesions on atrial leaflet surface
- Aortic insufficiency: Produces vegetations on ventricular side
- Ventricular septal defects: Right-sided vegetations near the orifice
Special Considerations
1. Culture-negative endocarditis often caused by:
- Coxiella burnetii
- Brucella species
- Tropheryma whipplei
- --
Beyond the Tutorial
Diagnostic Approach
1. Duke criteria: Major criteria include positive blood cultures and echocardiographic evidence of vegetations.
2. Blood cultures: Gold standard for diagnosis; must be taken before antibiotic therapy.
3. Echocardiography: Transthoracic (TTE) and transesophageal (TEE) are primary imaging modalities.
Clinical Manifestations
1. Fever: Present in >90% of cases.
2. Janeway lesions: Non-tender, erythematous macules on palms and soles.
3. Osler nodes: Painful, tender nodules on fingertips or toes.
4. Roth spots: Retinal hemorrhages with pale centers.
5. Splinter hemorrhages: Linear hemorrhages under nails.
Treatment Principles
1. Antibiotic therapy: Based on culture results and antibiotic susceptibility testing.
2. Surgical indications: Heart failure, uncontrolled infection, prevention of embolic events.
3. Prophylaxis: Limited to high-risk patients undergoing specific procedures.