
PANCE - Small Vessel Vasculitis
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for PANCE from the Small Vessel Vasculitis tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
 5. Eosinophilic granulomatosis with polyangiitis (EGPA):
5. Eosinophilic granulomatosis with polyangiitis (EGPA):
 6. Microscopic polyangiitis (MPA):
6. Microscopic polyangiitis (MPA):
- --
VITAL FOR PANCE
General Principles of Vasculitis
1. Small vessel vasculitides involve arterioles, venules, and capillaries, causing necrosis, ischemia, and organ dysfunction.
2. Common systemic features: fever, weight loss, fatigue, arthralgia, and palpable purpura.
3. Corticosteroids are the mainstay of initial treatment for all serious vasculitides, often combined with immunosuppressants if there is major organ involvement.
ANCA-Associated Small Vessel Vasculitides
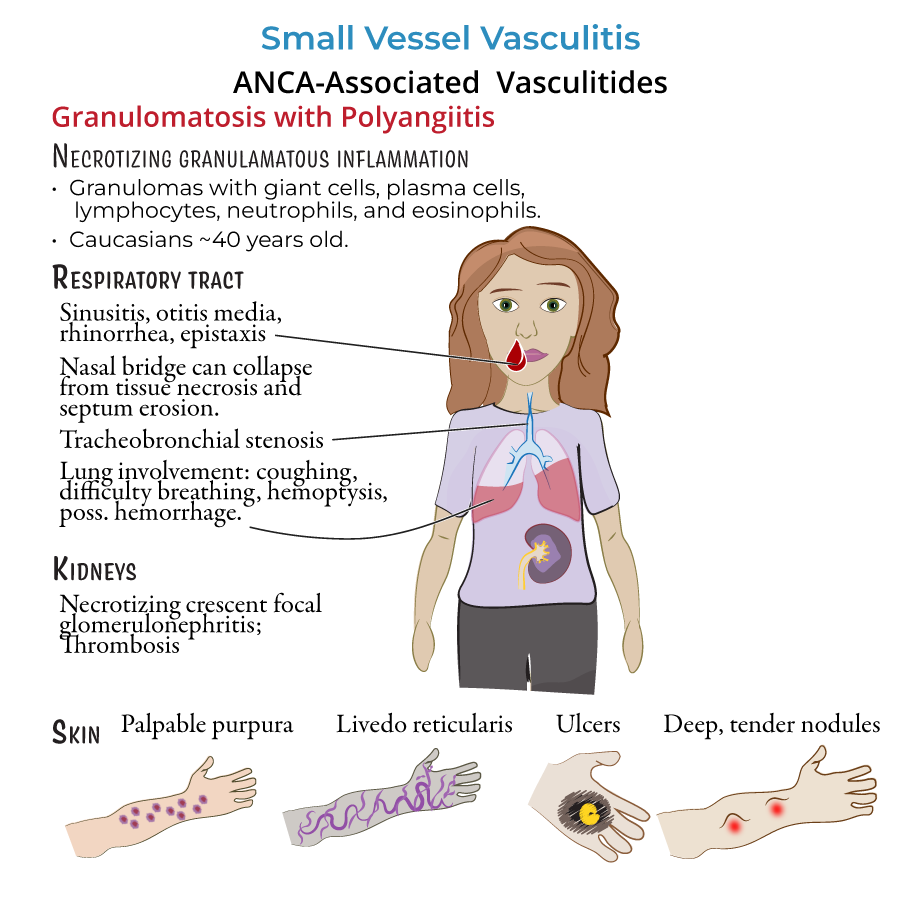
4. Granulomatosis with polyangiitis (GPA):
- Involves ENT, lungs, and kidneys.
- Classic findings:
- Chronic sinusitis, otitis media, nasal septal perforation (saddle-nose deformity).
- Pulmonary symptoms: cough, hemoptysis, cavitary lung nodules.
- Renal involvement: rapidly progressive glomerulonephritis (RPGN).
- c-ANCA positive (PR3-ANCA).
- Chest X-ray/CT: nodular cavitations.
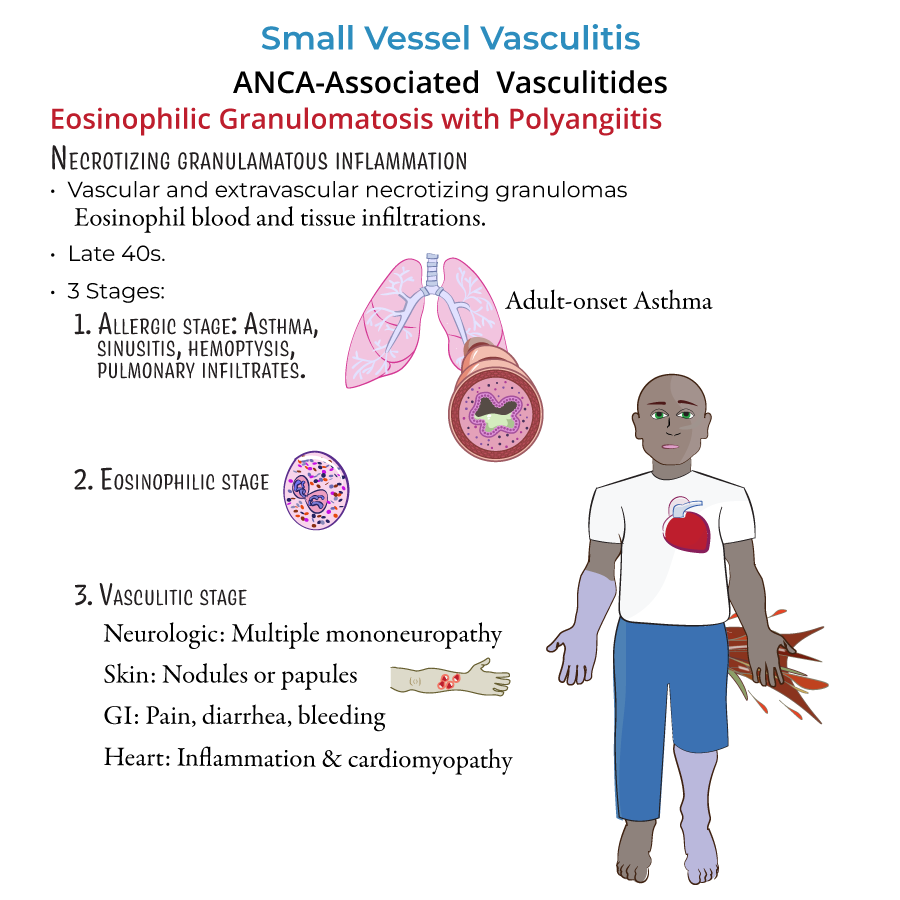
5. Eosinophilic granulomatosis with polyangiitis (EGPA):
- Triad: asthma, eosinophilia, vasculitis.
- Phases:
- Allergic (asthma, rhinitis).
- Eosinophilic (eosinophilic pneumonia).
- Vasculitic (mononeuritis multiplex, cardiac involvement).
- p-ANCA positive (MPO-ANCA).
- Cardiac involvement is the leading cause of mortality.
6. Microscopic polyangiitis (MPA):
- Necrotizing vasculitis without granulomas.
- Presents with glomerulonephritis and/or alveolar hemorrhage.
- p-ANCA positive.
- --
HIGH YIELD
Non-ANCA Small Vessel Vasculitides
1. IgA Vasculitis (Henoch-Schönlein Purpura):
- Most common small vessel vasculitis in children.
- Clinical tetrad:
- Palpable purpura (lower extremities, buttocks).
- Arthralgia.
- Abdominal pain (GI bleeding).
- Renal disease (IgA nephropathy).
- Preceded by upper respiratory infections.
- Management:
- Supportive care for mild cases.
- Corticosteroids for severe GI or renal involvement.
- Caused by cryoglobulin precipitation at cold temperatures.
- Associated with chronic Hepatitis C.
- Symptoms:
- Palpable purpura.
- Arthralgias.
- Glomerulonephritis.
- Diagnosis:
- Positive serum cryoglobulins.
- Low complement levels (especially C4).
- Management:
- Treat underlying Hepatitis C.
- Immunosuppression for severe cases.
- Small vessel vasculitis may be a late complication of systemic lupus erythematosus or rheumatoid arthritis.
- Presents with skin ulcers, glomerulonephritis, and neurologic symptoms.
- --
Beyond the Tutorial
Diagnostic Testing and Monitoring
1. ANCA Testing:
- c-ANCA (anti-PR3) → GPA.
- p-ANCA (anti-MPO) → MPA and EGPA.
- GPA: necrotizing granulomatous inflammation.
- MPA: necrotizing inflammation without granulomas.
- EGPA: eosinophilic infiltrates and granulomas.
- Chest CT for GPA shows nodules, cavitations.
- Chest imaging in MPA may show diffuse alveolar infiltrates if pulmonary hemorrhage is present.
Treatment Pearls
4. GPA and MPA:
- Induction: corticosteroids plus rituximab or cyclophosphamide.
- Maintenance: azathioprine, methotrexate, or rituximab.
- Mild: corticosteroids alone.
- Severe: corticosteroids plus cyclophosphamide or IL-5 inhibitors (e.g., mepolizumab).
- Initiate antiviral therapy first in Hepatitis C–positive patients.
- Immunosuppression reserved for severe, life-threatening cases.
- Monitor renal function closely, especially in adults.
Complications to Monitor
8. GPA:
- Pulmonary hemorrhage.
- End-stage renal disease.
- Heart failure secondary to myocarditis.
- Chronic kidney disease and peripheral neuropathy.
- Progressive renal impairment in adults.