
PANCE - Myocardial Infarction
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for Physician Assistant National Certifying Examination (PANCE) from the Myocardial Infarctions: Diagnosis & Treatment tutorial, focusing on clinical recognition, diagnosis, and management that are essential for certification. See the tutorial notes for further details and relevant links.
 3. Cardiac biomarkers:
Below is information not explicitly contained within the tutorial but important for the Physician Assistant National Certifying Examination.
3. Cardiac biomarkers:
Below is information not explicitly contained within the tutorial but important for the Physician Assistant National Certifying Examination.
- --
VITAL FOR PANCE
Epidemiology & Risk Factors
1. Global trends: Incidence of myocardial infarctions is declining in high-income countries but rising in middle- and low-income countries.
2. Demographic patterns: Incidence after age 35, from highest to lowest: Black males > Black females > White males > White females.
3. Age and gender differences: MI occurs approximately 10 years earlier in men than in women, possibly related to risk factors such as smoking and hyperlipidemia.
4. Mortality disparities: Although mortality rates have declined overall, they remain higher in women than in men, especially for young and/or minority women.
5. Modifiable risk factors: Dyslipidemia, diabetes mellitus, hypertension, smoking (possibly including daily use of e-cigarettes), obesity, psychosocial stress, alcohol consumption, poor diet (low in fruits and vegetables).
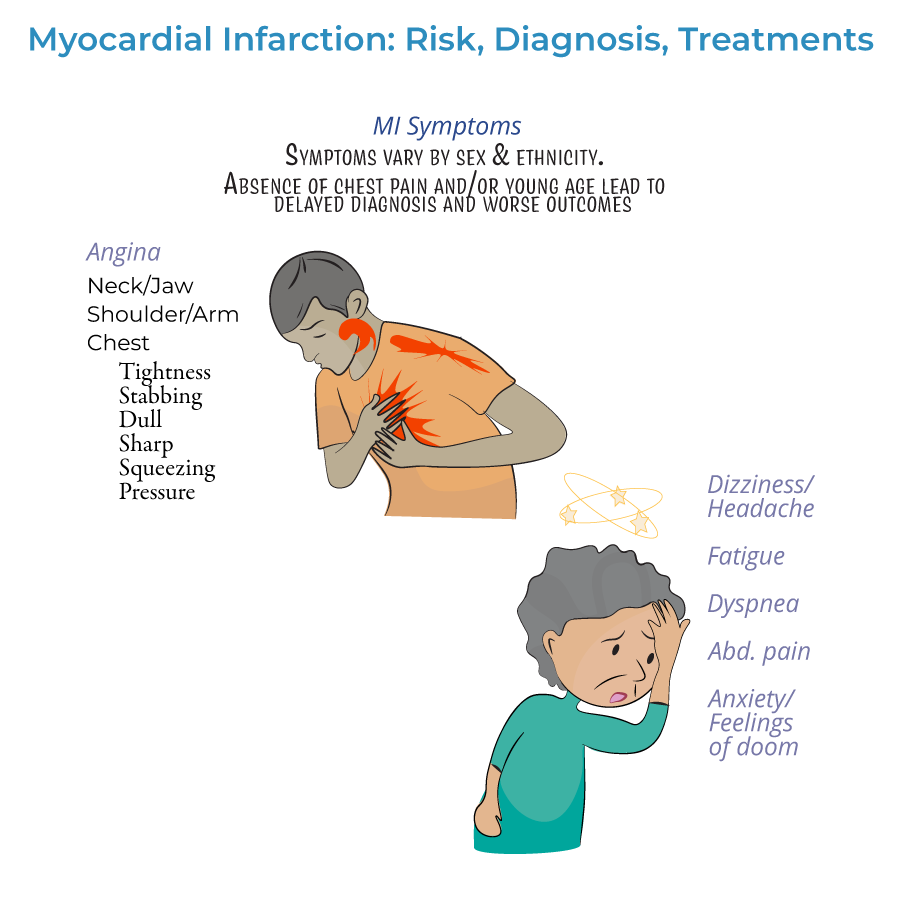
Clinical Presentation
1. Definition: Myocardial infarction is defined as myocardial injury with ischemia.
2. Presentation types:
- Prodromal symptoms: May occur days, weeks, or even months prior to the heart attack
- Acute symptoms: Experienced at the time of the event
- Silent MI: No noticeable symptoms
Diagnostic Approach
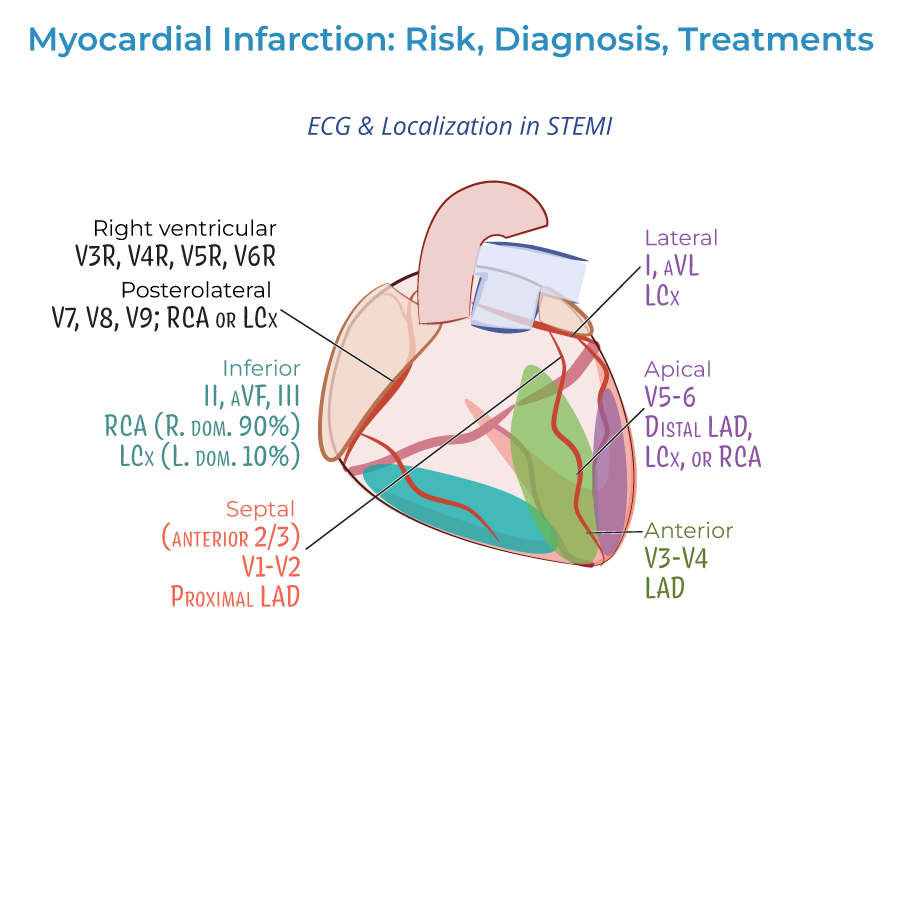
1. ECG evaluation:
- Should be administered as soon as possible when MI is suspected
- Should be re-administered frequently to observe the evolution of the infarction
- Distinguishes between ST-segment elevated (STEMI) or Non-ST elevated (NSTEMI) myocardial infarctions
- Q-wave abnormalities may indicate size/location of current MI or prior MI
- Lateral infarction: Leads I and aVL; left circumflex artery
- Apical infarction: Leads V5 and V6; left circumflex or right coronary arteries
- Anterior infarction: Leads V3 and V4; left anterior descending artery
- Anterior septal infarction: Leads V1 and V2; proximal left anterior descending artery
- Inferior infarction: Leads II, aVF, and III; right coronary artery or left circumflex artery
- Right ventricular infarction: Requires additional leads V3R through V6R
- Posterolateral infarction: Requires additional leads V7-V9; right coronary or left circumflex artery
3. Cardiac biomarkers:
- Essential for diagnosis, especially cardiac troponin
- Help distinguish between NSTEMI and unstable angina (only NSTEMI is associated with rising/falling troponin levels)
- Both cardiac troponin I and CK-MB peak within 24 hours of MI and fall to normal levels over time
Treatment Principles
1. Time-sensitive approach: Treatment should begin as soon as possible, ideally before hospital arrival, to reduce the extent of myocardial necrosis.
2. Pre-hospital treatment:
- Oxygen administration when oxygen saturation is less than 90%
- Aspirin for antiplatelet effects
- Nitrates for chest pain (morphine is an option if nitrates are ineffective)
- Vary by severity of infarction
- Include percutaneous coronary intervention (angioplasty), coronary bypass grafting, or fibrinolytic drugs
- STEMI patients should receive emergency PCI; if unavailable, fibrinolytic drugs must be given as soon as possible
- STEMI: Emergency PCI recommended (if unavailable, immediate fibrinolytics)
- NSTEMI: Unstable, complicated cases require immediate PCI/CABG; uncomplicated cases may wait longer with possible medical management only
- Fibrinolytic therapy: Generally not recommended for NSTEMI (risks outweigh benefits)
- Antiplatelets (aspirin, clopidogrel, or others)
- Anticoagulation drugs (unfractionated or low molecular weight heparin)
- Beta-blockers (or calcium-channel blockers)
- Statins
- ACE-inhibitors
Long-term Management
1. Risk factor modification: Long-term treatment focuses on reducing risk factors through improved diet and exercise.
2. Medical management: Ongoing medications to manage hypertension and hyperlipidemia.
3. Follow-up care: Regular monitoring for complications and progression to heart failure.
4. Patient education: Many patients, especially women, are unaware of risk factors and symptoms—education is a critical obstacle to prevention and treatment.
5. Secondary prevention: Aggressive risk factor management to prevent recurrent events.
- --
HIGH YIELD
Clinical Recognition Pearls
1. Atypical presentation awareness: Not all patients experience classic angina—absence should not exclude MI diagnosis.
2. Prodromal recognition: Symptoms in the days to months before acute MI may include fatigue, sleep disturbances, or vague discomfort.
3. Silent MI risk: Higher in diabetics and elderly patients—maintain high index of suspicion.
4. Gender differences: Women often present with more subtle or atypical symptoms and have worse outcomes.
5. Age considerations: Though MI occurs approximately 10 years earlier in men, young patients should not be excluded from consideration.
ECG Interpretation Essentials
1. Evolution monitoring: Serial ECGs track the progression of infarction and may reveal developing complications.
2. STEMI criteria: ST-segment elevation indicates transmural injury requiring immediate reperfusion.
3. NSTEMI patterns: ST depression or T-wave changes may indicate subendocardial ischemia.
4. Localization accuracy: Different lead changes correlate with specific coronary artery territories:
- Anterior (V3-V4): Left anterior descending artery
- Inferior (II, III, aVF): Right coronary artery (or less commonly left circumflex)
- Lateral (I, aVL): Left circumflex artery
Biomarker Utilization
1. Troponin significance: Key biomarker for diagnosis of myocardial infarction.
2. NSTEMI vs. unstable angina: Biomarker values help distinguish these conditions—only NSTEMI shows troponin elevation.
3. Temporal considerations: Both cardiac troponin I and CK-MB peak within 24 hours of MI.
4. Serial measurements: More valuable than single determinations for diagnosis and prognosis.
5. Interpretation context: Always integrate biomarker results with clinical presentation and ECG findings.
Treatment Decision-Making
1. Reperfusion timing: "Time is myocardium"—earlier treatment leads to better outcomes.
2. STEMI management: Emergency PCI preferred; if unavailable, immediate fibrinolytic therapy.
3. Pre-hospital initiation: Early aspirin, nitrates, and oxygen (when indicated) can limit infarct size.
4. NSTEMI approach: Risk stratification guides timing of invasive management—unstable patients need immediate intervention.
5. Pharmacotherapy selection: Evidence-based combinations of antiplatelets, anticoagulants, beta-blockers, statins, and ACE inhibitors.
Special Populations Considerations
1. Women: Higher mortality rates, more atypical presentations, later age of onset (approximately 10 years).
2. Minority patients: Black males have highest incidence after age 35, followed by Black females.
3. Young patients: Often missed or delayed diagnosis due to low clinical suspicion.
4. Elderly: May present with dyspnea or fatigue rather than chest pain.
5. Awareness disparities: Many patients, especially women, lack knowledge about risk factors and symptoms—patient education is crucial.
- --
Beyond the Tutorial
Differential Diagnosis
1. Acute coronary syndrome: STEMI, NSTEMI, and unstable angina differentiation.
2. Non-ACS cardiac causes: Myocarditis, pericarditis, cardiomyopathy, aortic dissection.
3. Pulmonary causes: Pulmonary embolism, pneumonia, pneumothorax, pleuritis.
4. Gastrointestinal conditions: Esophageal spasm, GERD, peptic ulcer, pancreatitis, cholecystitis.
5. Other considerations: Musculoskeletal pain, herpes zoster, anxiety/panic disorder.
Risk Stratification Tools
1. TIMI Risk Score: Predicts 14-day outcomes in ACS patients.
2. GRACE Risk Score: Predicts in-hospital and 6-month mortality.
3. HEART Score: Stratifies chest pain patients in the emergency department.
4. CRUSADE Score: Assesses bleeding risk in ACS patients.
5. Ottawa Heart Failure Risk Scale: Identifies low-risk chest pain patients.
Advanced Treatment Considerations
1. P2Y12 inhibitor selection: Clinical factors influencing choice between clopidogrel, ticagrelor, and prasugrel.
2. Anticoagulation options: UFH, LMWH, fondaparinux based on clinical scenario.
3. Bleeding risk management: Balancing antiplatelet/anticoagulant therapy with bleeding risk.
4. Revascularization decisions: Culprit-only vs. complete revascularization in multivessel disease.
5. Special situations: Cardiogenic shock, mechanical complications, right ventricular infarction.
Post-MI Care
1. Cardiac rehabilitation: Evidence-based programs improving outcomes.
2. Secondary prevention optimization: Target goals for lipids, blood pressure, and glucose.
3. Medication adherence strategies: Patient education and barrier identification.
4. Return to activities: Evidence-based guidance for driving, exercise, and work.
5. Screening for depression: Associated with worse outcomes if untreated.
Team-Based Care Considerations
1. STEMI systems of care: PA role in regional networks and transfer protocols.
2. Quality metrics: Understanding core measures for MI care.
3. Transition of care: Discharge planning, medication reconciliation, follow-up arrangements.
4. Patient education: Symptom recognition, risk factor modification, medication adherence.
5. Community resources: Connecting patients with smoking cessation, cardiac rehabilitation, and support services.