
PANCE - Medium & Variable Vessel Vasculitis
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for PANCE from the Medium & Variable Size Vessel Vasculitis tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
- --
VITAL FOR PANCE
General Features of Vasculitis
1. Vasculitis causes blood vessel inflammation, leading to ischemia, necrosis, and organ dysfunction across multiple systems.
2. First-line treatment for vasculitides usually includes high-dose corticosteroids.
3. Systemic symptoms include fever, weight loss, arthralgias, myalgias, and fatigue.
Polyarteritis Nodosa (PAN)
4. PAN is a necrotizing vasculitis of medium-sized muscular arteries.
5. It causes multisystem involvement:
- Nervous system: Mononeuritis multiplex (asymmetric neuropathy)
- Renal: Hypertension, renal ischemia (NO glomerulonephritis)
- GI: Mesenteric ischemia, abdominal pain
- Skin: Livedo reticularis, ulcers, nodules, gangrene
- Biopsy shows necrotizing inflammation of medium arteries.
- Angiography shows microaneurysms and irregular vessel narrowing.
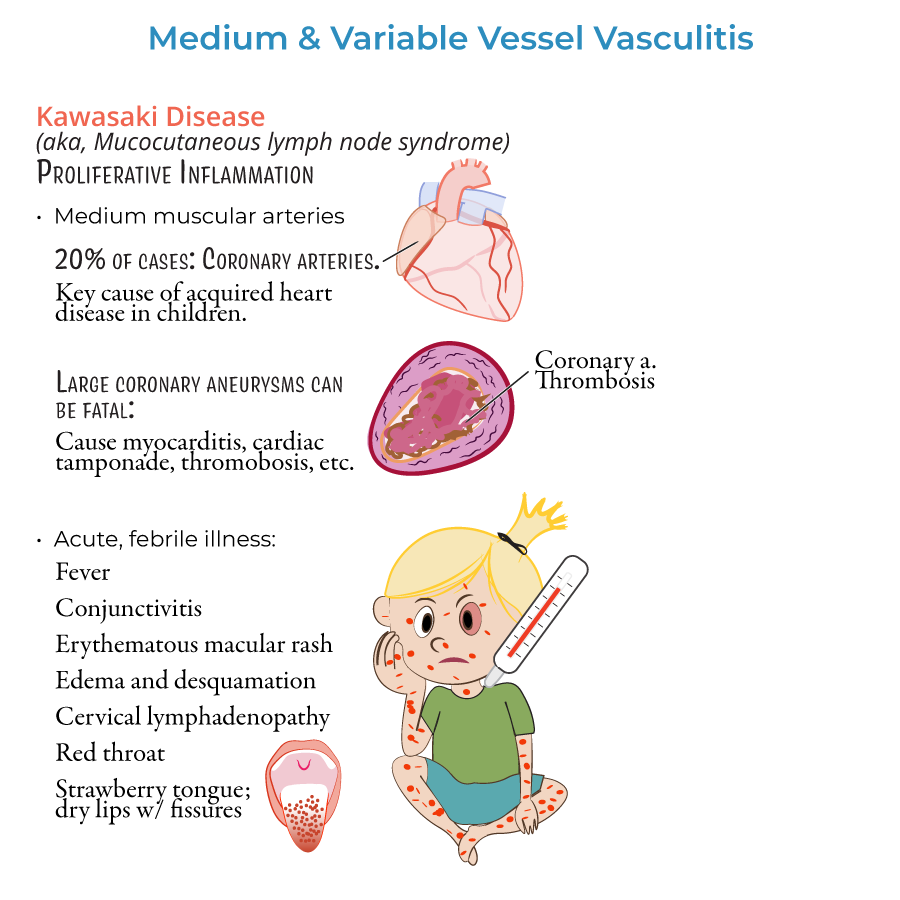
Kawasaki Disease
9. Kawasaki disease is a medium-vessel vasculitis affecting mostly children <5 years.
10. Diagnostic criteria:
- Fever ≥5 days plus ≥4 of 5 findings:
- Bilateral non-purulent conjunctivitis
- Oral mucosal changes (strawberry tongue, fissured lips)
- Polymorphous rash
- Extremity changes (swelling, desquamation)
- Cervical lymphadenopathy
- IVIG plus high-dose aspirin.
- Repeat echocardiograms at diagnosis and at 2–6 weeks to monitor coronary arteries.
- --
HIGH YIELD
Behçet Disease
1. Behçet disease is a variable-vessel vasculitis affecting arteries and veins of all sizes.
2. Clinical features:
- Oral aphthous ulcers
- Genital ulcers
- Ocular inflammation (anterior or posterior uveitis)
- Skin lesions (erythema nodosum, papulopustular rash)
- Corticosteroids during flares.
- Colchicine, azathioprine, or cyclosporine for maintenance and ocular disease.
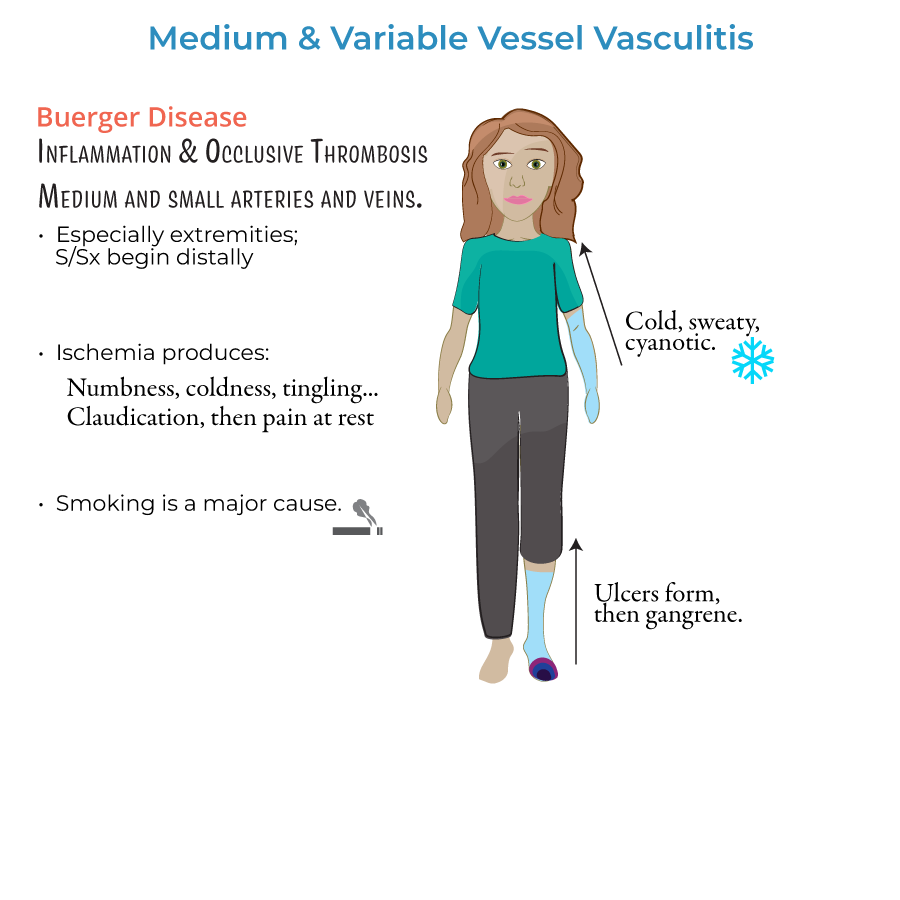
Buerger Disease (Thromboangiitis Obliterans)
6. Buerger disease affects small and medium arteries and veins, especially in young male smokers.
7. Key features:
- Distal ischemia causing claudication, coldness, numbness
- Ulceration and progression to gangrene
- Superficial thrombophlebitis
- Clinical suspicion in smokers.
- Arteriography shows corkscrew collaterals.
- Absolute smoking cessation is critical.
- No effective treatment if smoking continues.
Pathophysiology and Histology Summary
10. PAN: Transmural necrotizing inflammation of medium arteries, no pulmonary involvement, ANCA-negative.
11. Kawasaki: Proliferative inflammation of coronary arteries.
12. Behçet: Neutrophilic vasculitis of arteries and veins.
13. Buerger: Occlusive thrombus with preserved vessel wall architecture.
- --
Beyond the Tutorial
PAN Specifics
1. PAN spares the lungs, unlike GPA (Granulomatosis with Polyangiitis).
2. Cyclophosphamide is reserved for severe or refractory PAN not associated with hepatitis B.
Kawasaki Disease Notes
3. Coronary aneurysm formation occurs within the first few weeks; early IVIG prevents it.
4. Patients should avoid live vaccines (e.g., MMR, varicella) for 11 months post-IVIG therapy.
Behçet and Vascular Risk
5. DVTs and arterial thromboses can occur; important to monitor for signs of thrombotic complications.
Buerger Disease Special Considerations
6. Amputation may be necessary if tissue ischemia progresses despite smoking cessation.
7. Patients should be educated on good foot care and regular vascular checks.