
PANCE - Hypoparathyroidism & Calcium Imbalances
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for PANCE from the Parathyroid Hormone & Calcium Homeostasis tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
 Below is information not explicitly contained within the tutorial but important for PANCE & PANRE.
Below is information not explicitly contained within the tutorial but important for PANCE & PANRE.
- --
VITAL FOR PANCE
Parathyroid Hormone Physiology
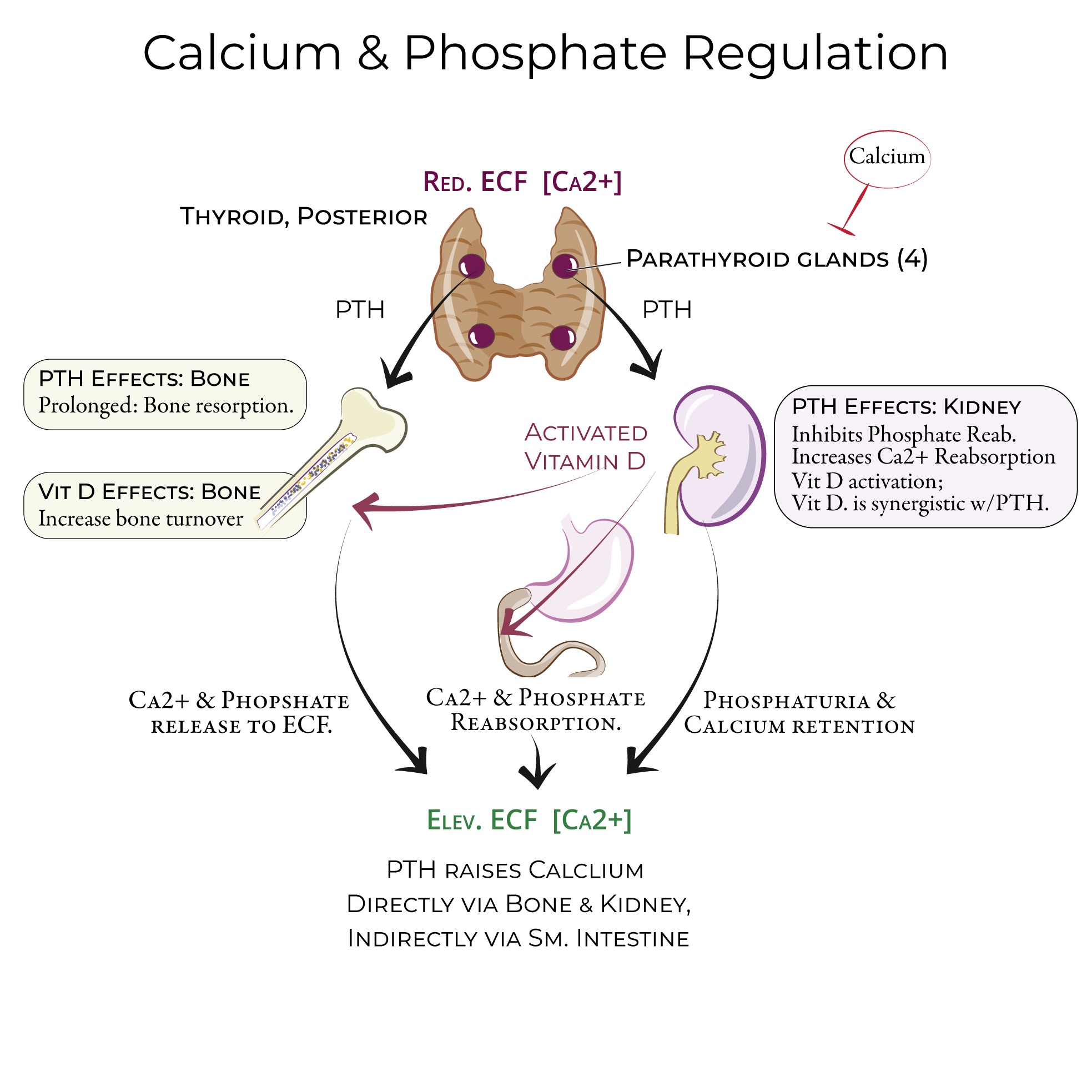
1. Parathyroid hormone increases ECF calcium levels.
2. Regulated by calcium and vitamin D.
3. Parathyroid hormone protects against hypocalcemia by causing calcium release from the bones and reabsorption from the kidneys.
4. In response to reduced extracellular calcium concentration, the parathyroid glands secrete parathyroid hormone (PTH).
5. The total effect of parathyroid hormone is to elevate extracellular calcium levels.
Hypoparathyroidism Essentials
1. Most often the result of surgical removal or damage to the parathyroid glands.
2. Other causes include autoimmune destruction (i.e., Autoimmune polyglandular syndrome type 1), congenital lack of functioning parathyroid glands, and very low magnesium levels.
3. Low parathyroid hormone leads to low levels of calcium and high levels of phosphate.
4. Two key signs of tetany in hypoparathyroidism: Chvostek sign and Trousseau's sign.
5. Treatments include activated Vitamin D and calcium supplements, possibly magnesium supplements.
Clinical Assessment Keys
1. Neuromuscular effects: Muscle weakness, Paresthesia, Cramping, Tetany.
2. Laryngospasms, bronchospasms, and stridor are also associated with hypoparathyroidism.
3. Typical reference blood calcium range is 2.2-2.6 mmol/L (8.6-10.3 mg/dL).
4. Chvostek sign: tapping the facial nerve produces facial muscle spasms.
5. Trousseau's sign: carpopedal spasm seen after a few minutes of wearing an inflated blood pressure cuff.
- --
HIGH YIELD
PTH Mechanisms and Function
1. Prolonged exposure to parathyroid hormone promotes resorption of old bone, releasing calcium and phosphate into extracellular fluid.
2. Episodic, transient binding of parathyroid hormone causes an increase in new bone synthesis.
3. Parathyroid hormone increases calcium reabsorption in the distal convoluted tubule of the nephrons.
4. It also stimulates activation of Vitamin D (activated form = 1,25(OH)2-VD).
5. Vitamin D acts on the nephron to increase reabsorption of calcium and phosphate.
6. In the small intestine, Vitamin D increases calcium and phosphate reabsorption.
7. In the bones, Vitamin D works with parathyroid hormone to facilitate skeletal remodeling.
8. If Vitamin D levels are high, parathyroid hormone secretion is inhibited.
Hypoparathyroidism Clinical Manifestations
Neuromuscular Effects
1. Muscle weakness
2. Paresthesia (tingling or burning, especially in the feet, hands, and around the mouth)
3. Cramping
4. Tetany
5. Laryngospasms, bronchospasms, and stridor
Other System Effects
1. Psychiatric effects: Irritability and confusion.
2. Cardiovascular effects: Include prolonged QT interval or heart failure.
3. Ocular: Cataracts
Diagnostic Signs
1. Chvostek sign: tapping the facial nerve (in the parotid gland/masseter muscle area) produces facial muscle spasms.
2. Trousseau's sign: carpopedal spasm seen after a few minutes of wearing an inflated blood pressure cuff (20 mmHg above systolic pressure). In the spasm, the patient will have flexed wrist, thumb, and metacarpophalangeal but hyperextended fingers.
Management Approaches
1. Activated Vitamin D and calcium supplements, possibly magnesium supplements.
2. Dietary recommendations: high in calcium (green leafy vegetables, legumes, fortified cereals) and low in phosphorous (less meat, soft drinks, and dairy products).
Related Disorders
1. Pseudohypoparathyroidism: Patients present with signs and symptoms associated with hypoparathyroidism but normal or elevated levels of parathyroid hormone – these patients have hormone resistance in the target organs.
Calcium Imbalances - Additional Causes
Hypercalcemia
1. Disorders that cause excessive bone resorption: Cancers, Paget disease, hyperthyroidism, Familial hypocalciuric hypercalcemia, Vitamin D toxicity.
2. Disorders that cause excessive gastrointestinal calcium absorption: Sarcoidosis, other granulomatous diseases.
3. Drugs that increase extracellular calcium, including lithium and thiazide diuretics.
Hypocalcemia
1. Vitamin D deficiency or resistance (including antiseizure drugs that alter vitamin D metabolism)
2. Pancreatitis
3. Magnesium imbalances
- --
Beyond the Tutorial
Advanced Clinical Management
1. Acute management of symptomatic hypocalcemia: IV calcium gluconate, monitoring protocols
2. Management of refractory hypoparathyroidism: recombinant parathyroid hormone therapy
3. Long-term monitoring parameters for patients on calcium and vitamin D supplementation
Primary Hyperparathyroidism
1. Clinical presentation: "stones, bones, abdominal groans, and psychic moans"
2. Laboratory findings: elevated calcium with inappropriately normal or elevated PTH
3. Localization techniques for parathyroid adenomas: ultrasound, sestamibi scan
4. Indications for surgical intervention versus medical management
Special Populations
1. Chronic kidney disease: pathophysiology of secondary hyperparathyroidism
2. Bariatric surgery patients: altered calcium absorption and monitoring needs
3. Pregnancy considerations: physiologic adaptations and management approaches
4. Pediatric patients: congenital hypoparathyroidism and calcium disorders