
SIADH for NP
Start your One-Week Free Trial
Already subscribed? Log in »
Syndrome of Inappropriate Antidiuretic Hormone (SIADH) for the Nurse Practitioner Licensing Exam
- Pathophysiology
- Excess ADH Secretion: SIADH involves excessive secretion of antidiuretic hormone (ADH), leading to increased water reabsorption by the kidneys despite normal or low plasma osmolality.
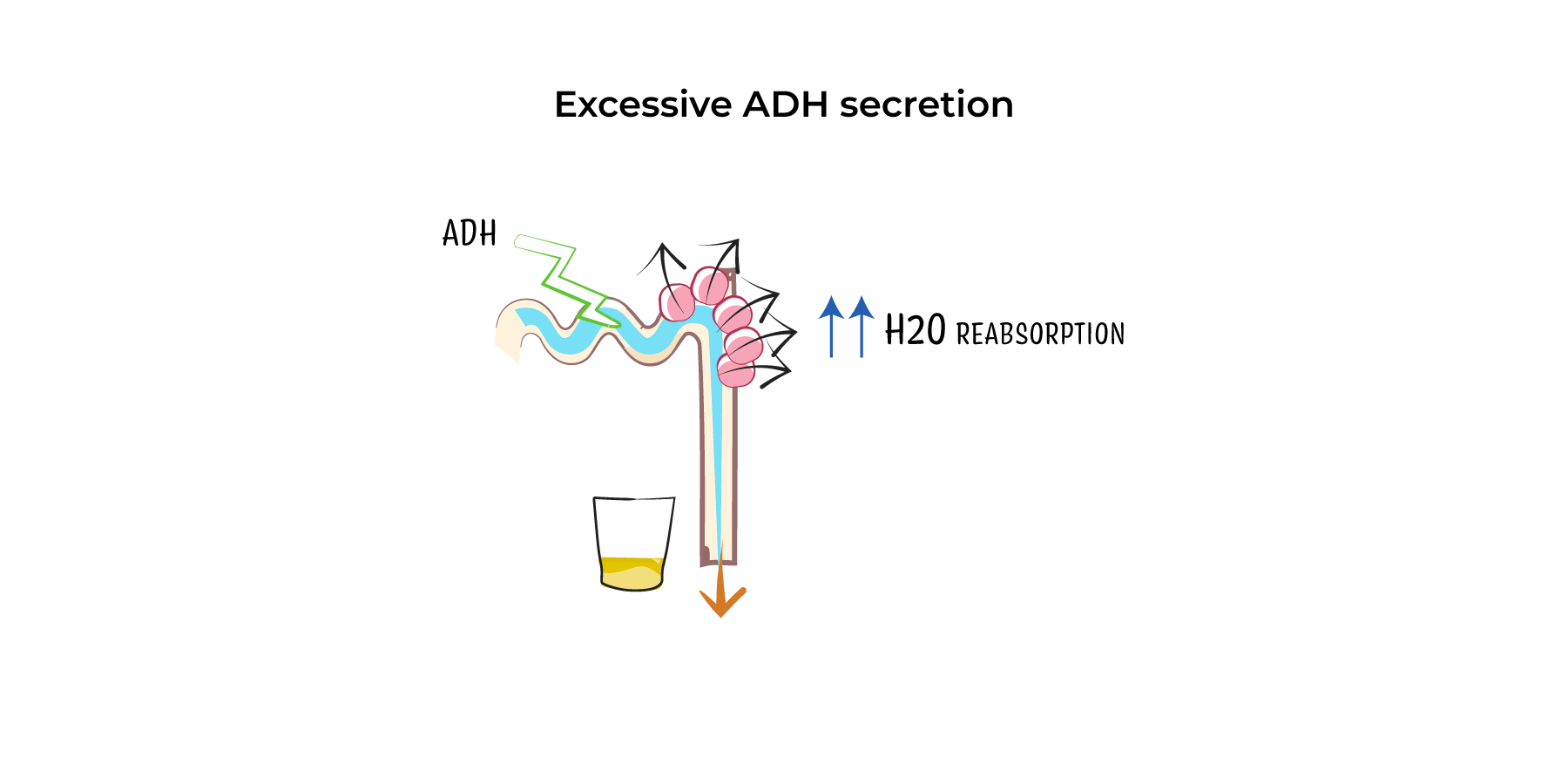
- Hyponatremia: The retained water dilutes plasma sodium levels, causing hyponatremia and low plasma osmolality. However, urine remains inappropriately concentrated (high urine osmolality).
- No Edema: Despite water retention, patients are usually euvolemic without signs of edema or hypervolemia.
- Etiology
- CNS Disorders: Head trauma, stroke, meningitis, and brain tumors can disrupt ADH regulation.
- Pulmonary Conditions: Pneumonia, tuberculosis, and chronic obstructive pulmonary disease (COPD) are common causes.
- Malignancies: Small-cell lung carcinoma is a classic cause due to ectopic ADH secretion.
- Medications: Drugs like SSRIs (e.g., fluoxetine), anticonvulsants (e.g., carbamazepine), and chemotherapy agents (e.g., cyclophosphamide) can induce SIADH.
- Post-Surgical: ADH secretion may increase after major surgery due to stress.
- Clinical Features
- Mild Hyponatremia (Na+ 130–135 mEq/L): Often asymptomatic but may cause fatigue, nausea, or headache.
- Moderate Hyponatremia (Na+ 120–129 mEq/L): Symptoms include confusion, lethargy, and muscle cramps.
- Severe Hyponatremia (Na+ <120 mEq/L): Neurological symptoms like seizures, altered mental status, and coma due to cerebral edema.
- Diagnosis
- Low Serum Sodium (<135 mEq/L) and Low Plasma Osmolality (<275 mOsm/kg).
- High Urine Osmolality (>100 mOsm/kg) despite hyponatremia.
- Elevated Urine Sodium (>20–30 mEq/L) with no signs of volume depletion or overload.
- Normal Renal, Thyroid, and Adrenal Function.
- Management
- Fluid Restriction: The primary treatment, limiting fluid intake to 500–1,000 mL/day.
- Hypertonic Saline (3%): For severe or symptomatic cases, correcting sodium levels slowly to avoid complications.
- Medications: Vasopressin receptor antagonists (e.g., tolvaptan) and, in refractory cases, demeclocycline to promote free water excretion.
Key Points
- Pathophysiology: SIADH is caused by excessive ADH secretion, leading to water retention and dilutional hyponatremia.
- Causes: Include CNS disorders, pulmonary conditions, small-cell lung carcinoma, and certain medications.
- Symptoms: Range from asymptomatic mild hyponatremia to severe neurological symptoms in cases of marked hyponatremia.
- Diagnosis: Hyponatremia with low plasma osmolality, high urine osmolality, and normal renal, thyroid, and adrenal function.
- Treatment: Fluid restriction is first-line, with hypertonic saline used for severe cases.