
NCLEX Focus - Heart Murmurs
Start your One-Week Free Trial
Already subscribed? Log in »
The following are high yield points from the Heart Murmurs tutorial to help you prepare for the NCLEX.
Review this Heart Murmurs flashcard for further details.
 Here's an NCLEX-focused summary of the Heart Murmurs tutorial, emphasizing high-yield facts directly derived from the provided material. This version highlights critical knowledge areas for test readiness and clinical reasoning.
A patient with known Marfan syndrome is being monitored for aortic valve dysfunction. What clinical change would suggest development of aortic insufficiency?
A nurse is auscultating a patient’s heart and hears a high-pitched, holosystolic murmur that lasts from S1 to S2, best heard at the apex. What condition is most likely causing this sound?
Which of the following hemodynamic changes is expected in a patient with aortic regurgitation?
A 15-year-old athlete presents with a mid-systolic click and high-pitched murmur that increases during the Valsalva maneuver. What is the most likely diagnosis?
Here's an NCLEX-focused summary of the Heart Murmurs tutorial, emphasizing high-yield facts directly derived from the provided material. This version highlights critical knowledge areas for test readiness and clinical reasoning.
A patient with known Marfan syndrome is being monitored for aortic valve dysfunction. What clinical change would suggest development of aortic insufficiency?
A nurse is auscultating a patient’s heart and hears a high-pitched, holosystolic murmur that lasts from S1 to S2, best heard at the apex. What condition is most likely causing this sound?
Which of the following hemodynamic changes is expected in a patient with aortic regurgitation?
A 15-year-old athlete presents with a mid-systolic click and high-pitched murmur that increases during the Valsalva maneuver. What is the most likely diagnosis?
NCLEX Focus
- --
NCLEX-Focused Summary: Heart Murmurs
- --
Fundamentals of Heart Murmurs
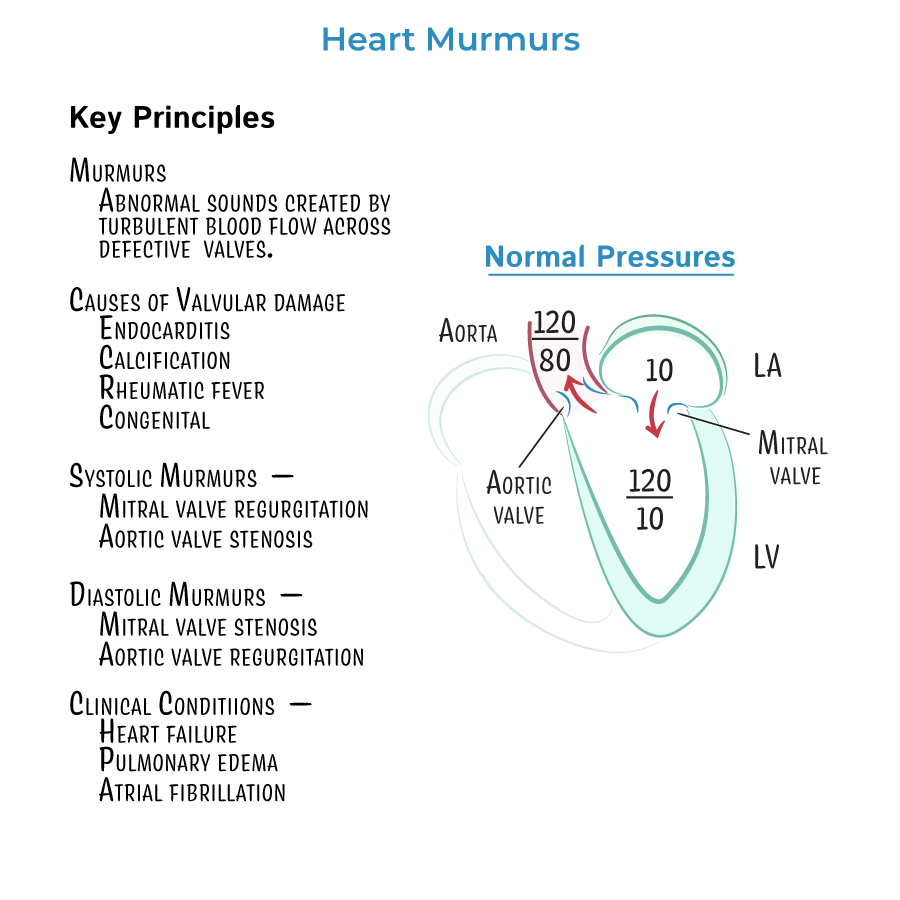
Heart murmurs = abnormal sounds from turbulent blood flow across defective valves.
Though echocardiography confirms diagnosis, auscultation remains an essential bedside skill.
Causes of murmurs include:
- Valvular calcification
- Infective endocarditis
- Rheumatic fever (post-streptococcal autoimmune)
- Congenital valve defects
- --
Hemodynamic Basics (Left Heart Reference)
Left atrial pressure: ~10 mmHg
Left ventricular pressure: 120 mmHg systolic / 10 mmHg diastolic
Aortic pressure: 120/80 mmHg
Murmurs result from abnormal pressure gradients and flow disruptions during the cardiac cycle.
- --
Mitral Valve Regurgitation
Murmur timing: Systole (holosystolic murmur from S1 to S2)
Phonocardiogram: High-pitched, steady sound
Hemodynamics:
- Blood leaks from LV to LA during systole
- ↑ LA pressure (high v-wave) → pulmonary congestion/edema
- ↑ LV preload due to increased return → LV dilation
- ↓ Aortic pressure (less forward stroke volume)
- --
Aortic Valve Regurgitation
Murmur timing: Diastole (after S2)
Phonocardiogram: High-pitched, early diastolic murmur
Hemodynamics:
- Blood leaks from aorta to LV during diastole
- ↑ LV preload → ↑ systolic pressure, ↓ diastolic pressure
- ↑ pulse pressure (wide gap between systolic/diastolic)
- ↑ LA pressure, risk of pulmonary congestion
- --
Mitral Valve Stenosis
Murmur timing: Diastole (after S2, with opening snap)
Phonocardiogram: Low-pitched murmur following an opening snap
Hemodynamics:
- Narrowed valve → ↑ LA pressure
- Atrial hypertrophy to push blood through stiff valve
- ↓ LV filling, ↓ preload, ↓ stroke volume
- ↓ Aortic pressure, ↓ cardiac output
- --
Aortic Valve Stenosis
Murmur timing: Systole
Phonocardiogram: Loud, harsh crescendo-decrescendo murmur
Hemodynamics:
- Stiff valve → ↓ aortic pressure during systole
- ↑ LV pressure to overcome stenosis → LV hypertrophy
- ↑ LA pressure → LA hypertrophy
- --
Clinical Correlations
Atrial hypertrophy from chronic pressure load → risk of atrial fibrillation
Heart failure and pulmonary edema can result from elevated left-sided pressures
Patent ductus arteriosus causes a continuous murmur, loudest at S2
- --
Mitral Valve Prolapse (MVP)
Murmur: Mid-systolic click + high-pitched systolic murmur
Common in: Marfan syndrome, Ehlers-Danlos, young females
Murmur increases with Valsalva (REDUCED preload accentuates leaflet prolapse)
Etiology: Myxomatous degeneration of mitral valve leaflets
Complications: Severe MVP can lead to mitral regurgitation, sudden cardiac death in athletes
Often asymptomatic, but requires monitoring
NCLEX Questions