
NCLEX - Thyroid Gland Pathophysiology
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for NCLEX-RN from the Thyroid Gland Pathophysiology tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
 2. Basic Pathology: Pathology can be broadly categorized as hyperthyroidism, which produces thyrotoxicosis, or hypothyroidism, which produces myxedema.
3. Goiter: Goiter = an enlarged thyroid gland. Goiter can be benign or a sign of underlying thyroid disease.
4. Common Causes in US:
Hyperthyroidism = Graves disease
Hypothyroidism = Hashimoto thyroiditis
Below is information not explicitly contained within the tutorial but important for NCLEX.
2. Basic Pathology: Pathology can be broadly categorized as hyperthyroidism, which produces thyrotoxicosis, or hypothyroidism, which produces myxedema.
3. Goiter: Goiter = an enlarged thyroid gland. Goiter can be benign or a sign of underlying thyroid disease.
4. Common Causes in US:
Hyperthyroidism = Graves disease
Hypothyroidism = Hashimoto thyroiditis
Below is information not explicitly contained within the tutorial but important for NCLEX.
- --
VITAL FOR NCLEX
Thyroid Disorder Assessment
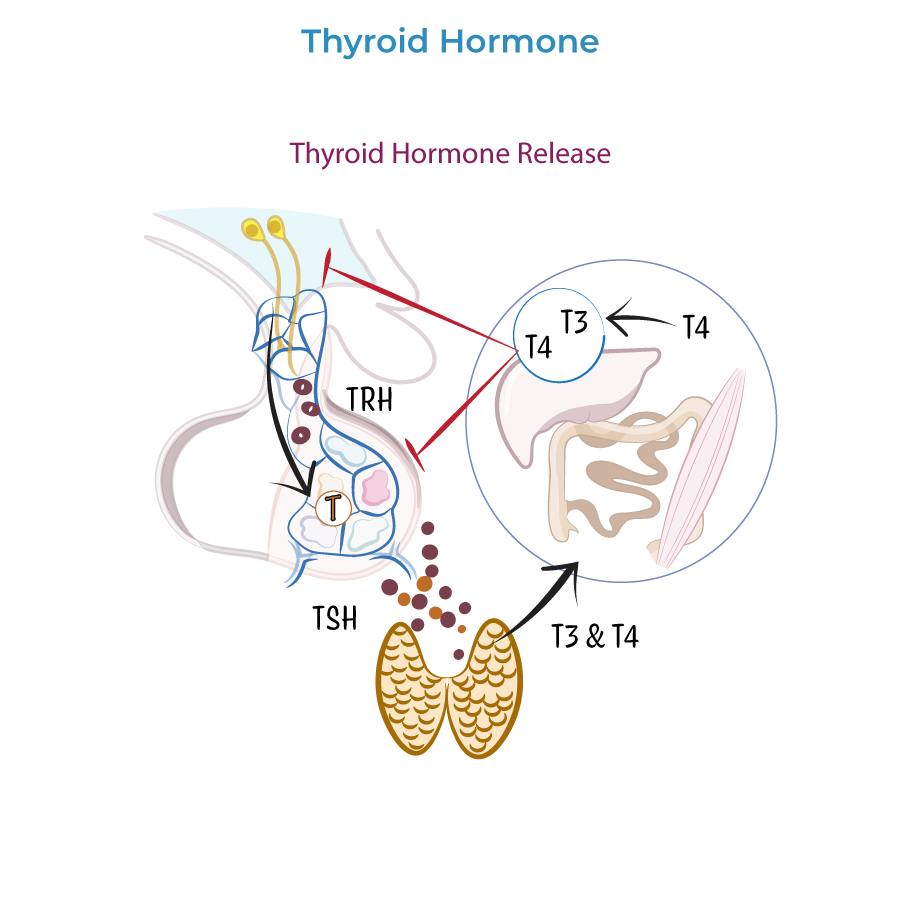
1. Thyroid Function: Thyroid hormones T3 and T4 are responsible for: CNS development in infants, Bone growth and maturation in children, Proper functioning in multiple organ systems in adults.
2. Basic Pathology: Pathology can be broadly categorized as hyperthyroidism, which produces thyrotoxicosis, or hypothyroidism, which produces myxedema.
3. Goiter: Goiter = an enlarged thyroid gland. Goiter can be benign or a sign of underlying thyroid disease.
4. Common Causes in US:
Hyperthyroidism = Graves disease
Hypothyroidism = Hashimoto thyroiditis
Key Assessment Findings
1. Vital Signs - Hyperthyroidism: Tachycardia with palpitations. Patients experience dyspnea and chest pain and have systolic hypertension.
2. Vital Signs - Hypothyroidism: Bradycardia with reduced cardiac output. Patients experience dyspnea on exertion and are at risk for hypoventilation.
3. Metabolic Signs - Hyperthyroidism: Heat intolerance with increased sweating; patients have elevated basal metabolic rate with weight loss.
4. Metabolic Signs - Hypothyroidism: Cold intolerance and reduced sweating; patients have lower basal metabolic rates with weight gain, and possibly hyponatremia.
Critical Assessment Differences
1. Neurological: Hyperthyroidism: hyperactivity, restlessness, anxiety, and insomnia. Patient have increased reflexes and fine motor tremors. Hypothyroidism has the opposite effects: patients are hypoactive, fatigued, and experience weakness and depressed mood with slow reflexes.
2. Integumentary: Hyperthyroidism: vasodilation produces warm, moist skin; hair is often fine (thin diameter). Hypothyroidism: patients have reduced blood flow with cool, dry skin. Hair is often coarse and brittle, and patients may have alopecia.
3. Gastrointestinal: Hyperthyroidism: more bowel movements, possibly with diarrhea, and appetite is increased. Hypothyroidism: constipation and reduced appetite.
- --
HIGH YIELD
System-Specific Assessment
Cardiovascular Assessment
1. Hyperthyroidism: tachycardia with palpitations. Patients experience dyspnea and chest pain and have systolic hypertension.
2. Hypothyroidism: bradycardia with reduced cardiac output. Patients experience dyspnea on exertion and are at risk for hypoventilation.
3. Chronotropic and inotropic effects on the heart (heart rate and contractility) are normal thyroid functions.
Neurological Assessment
1. Hyperthyroidism: hyperactivity, restlessness, anxiety, and insomnia. Patient have increased reflexes and fine motor tremors.
2. Hypothyroidism has the opposite effects: patients are hypoactive, fatigued, and experience weakness and depressed mood with slow reflexes.
3. Thyroid hormones maintain ventilatory responses to hypoxia and hypercapnia.
Musculoskeletal Assessment
1. Hyperthyroidism: breaks down proteins and muscles, producing proximal weakness with normal levels of creatine kinase.
2. Hypothyroidism also produces proximal weakness, but with myalgia; creatine kinase levels are often elevated.
3. Thyroid hormone promotes normal bone growth and development in children.
Gastrointestinal and Metabolic Assessment
1. Hyperthyroidism: more bowel movements, possibly with diarrhea, and appetite is increased.
2. Hypothyroidism: constipation and reduced appetite.
3. Hyperthyroidism: heat intolerance with increased sweating; patients have elevated basal metabolic rate with weight loss.
4. Hypothyroidism: cold intolerance and reduced sweating; patients have lower basal metabolic rates with weight gain, and possibly hyponatremia.
Integumentary Assessment
1. Hyperthyroidism: vasodilation produces warm, moist skin; hair is often fine (thin diameter).
2. Hypothyroidism: patients have reduced blood flow with cool, dry skin. Hair is often coarse and brittle, and patients may have alopecia. Nails are brittle.
3. Hypothyroidism is often characterized by nonpitting edema and puffy facies, due to water retention – thus its alternative name, myxedema.
Reproductive Assessment
1. Hyperthyroidism: irregular or reduced menstrual flow, gynecomastia, lower libido, and possibly reduced fertility.
2. Hypothyroidism: similar effects, but gynecomastia is not common.
Ocular Assessment
1. Both hyper- and hypothyroidism: can produce periorbital edema.
2. Hyperthyroidism is also associated with exophthalmos, aka, proptosis, which is characterized by 'bulging' eyeballs due to inflammation around the eyes.
3. Lid retraction can also occur in hyperthyroidism due to increased sympathetic stimulation of the muscles of the eyelid.
- --
Beyond the Tutorial
Nursing Considerations
1. Medication administration: Timing of levothyroxine (empty stomach), interactions with other medications.
2. Patient education: Importance of medication adherence, recognition of symptoms of hypo/hyperthyroidism.
3. Monitoring: Signs of treatment effectiveness or adverse effects.
Priority Nursing Diagnoses
1. Hyperthyroidism: Risk for decreased cardiac output, imbalanced nutrition, anxiety.
2. Hypothyroidism: Activity intolerance, constipation, ineffective thermoregulation.
3. Both conditions: Disturbed body image, risk for injury.
Emergency Management
1. Thyroid storm: Recognition of life-threatening hyperthyroidism, immediate interventions.
2. Myxedema coma: Recognition of severe hypothyroidism, supportive care measures.
3. Airway management: Considerations with thyroid enlargement causing tracheal compression.