
SIADH for ABIM
Start your One-Week Free Trial
Already subscribed? Log in »
Syndrome of Inappropriate Antidiuretic Hormone (SIADH) for the American Board of Internal Medicine Exam
- Pathophysiology
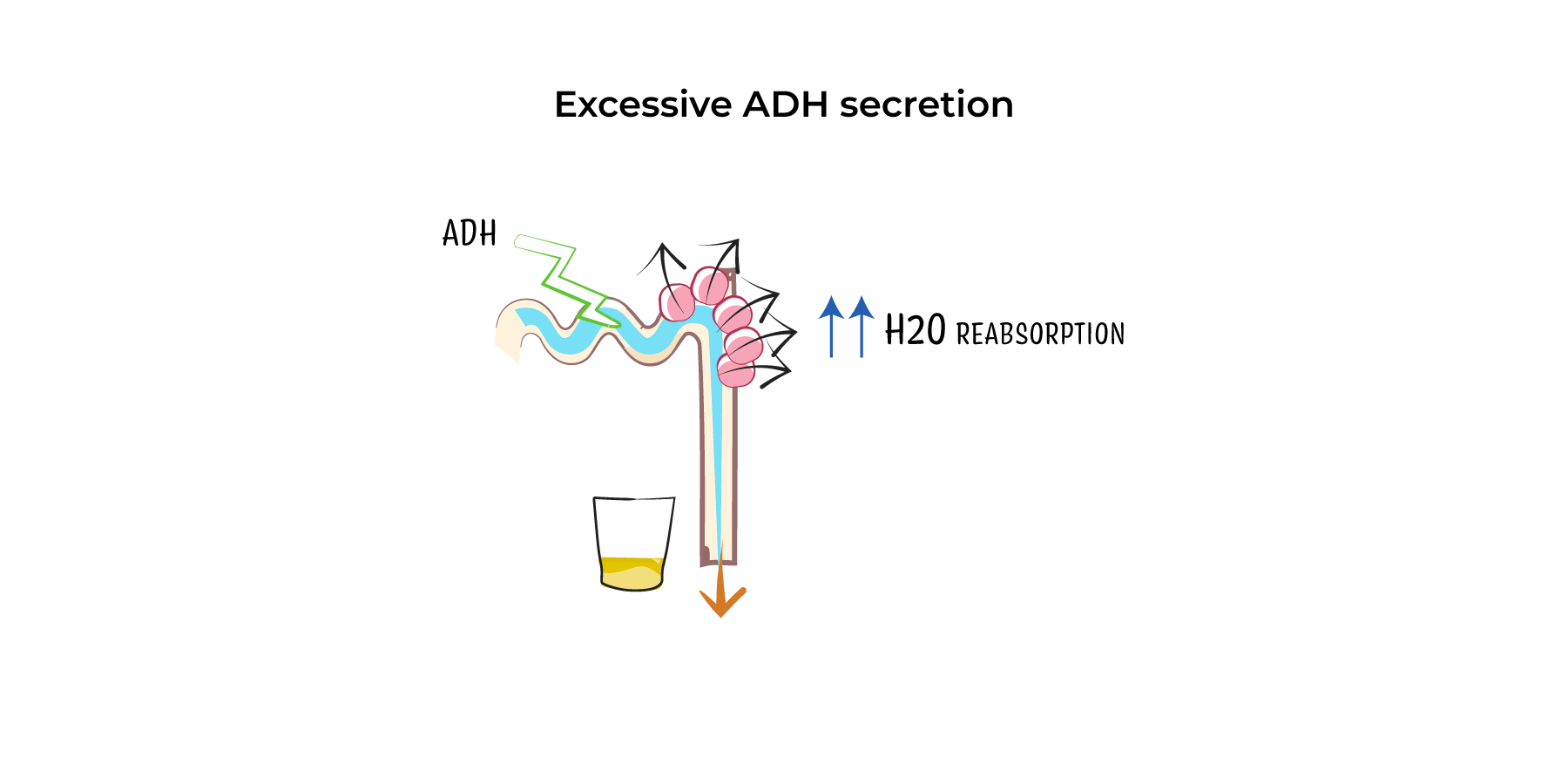
- Excessive ADH Secretion: ADH (antidiuretic hormone) promotes water reabsorption in the kidneys, concentrating the urine. In SIADH, excess ADH is secreted despite normal or low plasma osmolality, leading to impaired free water excretion.
- Water Retention and Hyponatremia: The retention of free water without proportional retention of sodium leads to dilutional hyponatremia. Plasma osmolality decreases, while urine osmolality remains inappropriately high.
- No Edema: Unlike other causes of hyponatremia, SIADH does not lead to peripheral edema because the water retention occurs intracellularly rather than in the extracellular space.
- Causes
- CNS Disorders: Head trauma, stroke, subarachnoid hemorrhage, meningitis, and encephalitis can disrupt the hypothalamic regulation of ADH.
- Malignancies: Certain tumors, especially small-cell lung carcinoma, produce ectopic ADH. Other cancers (e.g., pancreatic or prostate cancer) can also cause SIADH.
- Pulmonary Disorders: Pneumonia, tuberculosis, and lung abscesses can trigger SIADH. Mechanical ventilation may also stimulate ADH secretion.
- Medications:
- Antidepressants: SSRIs (e.g., fluoxetine) and tricyclics (e.g., amitriptyline).
- Antipsychotics: Drugs like haloperidol.
- Chemotherapy Agents: Vincristine and cyclophosphamide.
- Other Medications: NSAIDs, opioids, and carbamazepine.
- Post-Surgical State: SIADH can occur after major surgery due to stress-related ADH release.
- Idiopathic: In some cases, no identifiable cause is found.
- Clinical Features
- Symptoms of Hyponatremia:
- Mild Hyponatremia (Na+ 130–135 mEq/L): May be asymptomatic or present with nonspecific symptoms like fatigue, headache, nausea, and vomiting.
- Moderate Hyponatremia (Na+ 120–129 mEq/L): Can cause lethargy, confusion, dizziness, and muscle cramps.
- Severe Hyponatremia (Na+ <120 mEq/L): Leads to neurologic symptoms such as seizures, altered mental status, and coma, due to cerebral edema from water shifts into brain cells.
- Other Symptoms:
- Weight Gain Without Edema: Water retention leads to weight gain, but without peripheral edema.
- Decreased Urine Output: Concentrated urine despite low plasma osmolality.
- Diagnosis
- Hyponatremia with Low Plasma Osmolality: Serum sodium <135 mEq/L and plasma osmolality <275 mOsm/kg.
- Inappropriately High Urine Osmolality: Urine osmolality >100 mOsm/kg, despite hypotonic plasma.
- Urine Sodium Concentration >20–30 mEq/L: Demonstrates renal sodium loss due to the kidneys' response to excess water.
- Euvolemia: Clinical assessment should show no signs of volume depletion (e.g., dry mucous membranes, orthostatic hypotension) or hypervolemia (e.g., edema, ascites).
- Normal Adrenal, Thyroid, and Renal Function: Rule out other causes of hyponatremia, such as adrenal insufficiency or hypothyroidism. Normal renal function excludes chronic kidney disease as the cause of water retention.
- Differential Diagnosis
- Other Causes of Hyponatremia:
- Hypovolemic Hyponatremia: Occurs due to true volume depletion (e.g., vomiting, diarrhea, diuretics) with low urine sodium (<20 mEq/L).
- Hypervolemic Hyponatremia: Caused by heart failure, cirrhosis, or nephrotic syndrome, with signs of fluid overload.
- Adrenal Insufficiency: Can cause hyponatremia with low cortisol levels.
- Hypothyroidism: Severe hypothyroidism can impair free water excretion.
- Management
- Treatment of Underlying Cause: Address the primary cause of SIADH, such as removing an offending medication or treating a lung infection or tumor.
- Fluid Restriction:
- First-Line Therapy: Restrict free water intake to 500–1,000 mL/day to prevent further water retention.
- Hypertonic Saline (3%):
- Indicated for severe or symptomatic hyponatremia, especially when neurologic symptoms are present (e.g., seizures, coma).
- Slow Correction: Increase serum sodium by no more than 4–6 mEq/L in the first 24 hours to avoid osmotic demyelination syndrome (ODS), a serious complication resulting from overly rapid correction.
- Oral Salt Tablets or Loop Diuretics:
- Used in moderate cases to increase solute intake or promote free water excretion.
- Furosemide: Given to increase urinary water excretion while minimizing sodium loss.
- Vasopressin Receptor Antagonists (Vaptans):
- Tolvaptan and Conivaptan: Block ADH action at the V2 receptor, leading to increased free water excretion (aquaresis).
- Indications: Considered for chronic, refractory SIADH in cases where fluid restriction alone is ineffective.
- Demeclocycline:
- An older tetracycline antibiotic that induces nephrogenic diabetes insipidus, thus promoting free water excretion.
- Typically used in refractory cases but limited by potential nephrotoxicity.
- Monitoring and Follow-Up
- Serum Sodium Monitoring: Frequent monitoring is required, especially during treatment, to prevent rapid changes in sodium levels.
- Neurologic Monitoring: Close observation for signs of neurologic improvement or deterioration, particularly in severe hyponatremia.
- Long-Term Management: In chronic SIADH, ongoing fluid restriction or medications (e.g., vaptans) may be necessary to maintain normal sodium levels.
- Complications
- Severe Hyponatremia: Can lead to seizures, coma, and potentially fatal complications if not treated.
- Osmotic Demyelination Syndrome (ODS): Occurs with overly rapid correction of hyponatremia, causing demyelination of pontine neurons. Symptoms include quadriplegia, dysphagia, dysarthria, and altered consciousness, which may be irreversible.
- Chronic Hyponatremia: Long-term effects may include cognitive dysfunction and gait disturbances, especially in elderly patients.
Key Points
- Pathophysiology: SIADH results from excessive ADH secretion, leading to free water retention and dilutional hyponatremia.
- Etiology: Causes include CNS disorders, malignancies (especially small-cell lung carcinoma), medications (SSRIs, antipsychotics), and pulmonary infections.
- Clinical Features: Hyponatremia causes nonspecific symptoms like headache, nausea, and confusion, with severe cases resulting in seizures and coma.
- Diagnosis: Based on hyponatremia with low plasma osmolality, high urine osmolality, and euvolemia, excluding other causes of hyponatremia.
- Management: Includes fluid restriction, hypertonic saline for severe cases, and vasopressin receptor antagonists (vaptans) for chronic, refractory SIADH.
- Complications: Rapid correction of hyponatremia can lead to osmotic demyelination syndrome, a potentially irreversible condition.