
ABIM - Medium & Variable Vessel Vasculitis
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for ABIM from the Medium & Variable Size Vessel Vasculitis tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
- --
VITAL FOR ABIM
General Concepts of Vasculitis
1. Vasculitis is characterized by blood vessel inflammation, leading to tissue ischemia, necrosis, and multi-organ dysfunction.
2. Systemic signs include fever, fatigue, weight loss, arthralgia, and myalgia.
3. High-dose corticosteroids are the mainstay of treatment for most clinically significant vasculitides.
Polyarteritis Nodosa (PAN)
4. PAN is a necrotizing vasculitis affecting medium-sized muscular arteries.
5. Clinical manifestations:
- Peripheral neuropathy: Mononeuritis multiplex (asymmetric motor and sensory deficits)
- Renal ischemia: Hypertension and renal dysfunction (but no glomerulonephritis)
- Gastrointestinal ischemia: Abdominal pain, nausea, risk of mesenteric infarction
- Skin involvement: Livedo reticularis, subcutaneous nodules, ulcers
- Angiography: Shows microaneurysms and stenotic lesions.
- Biopsy: Shows transmural necrotizing inflammation of medium arteries.
- High-dose corticosteroids
- Antivirals and plasma exchange if HBV-positive
- Consider cyclophosphamide for severe, refractory cases.
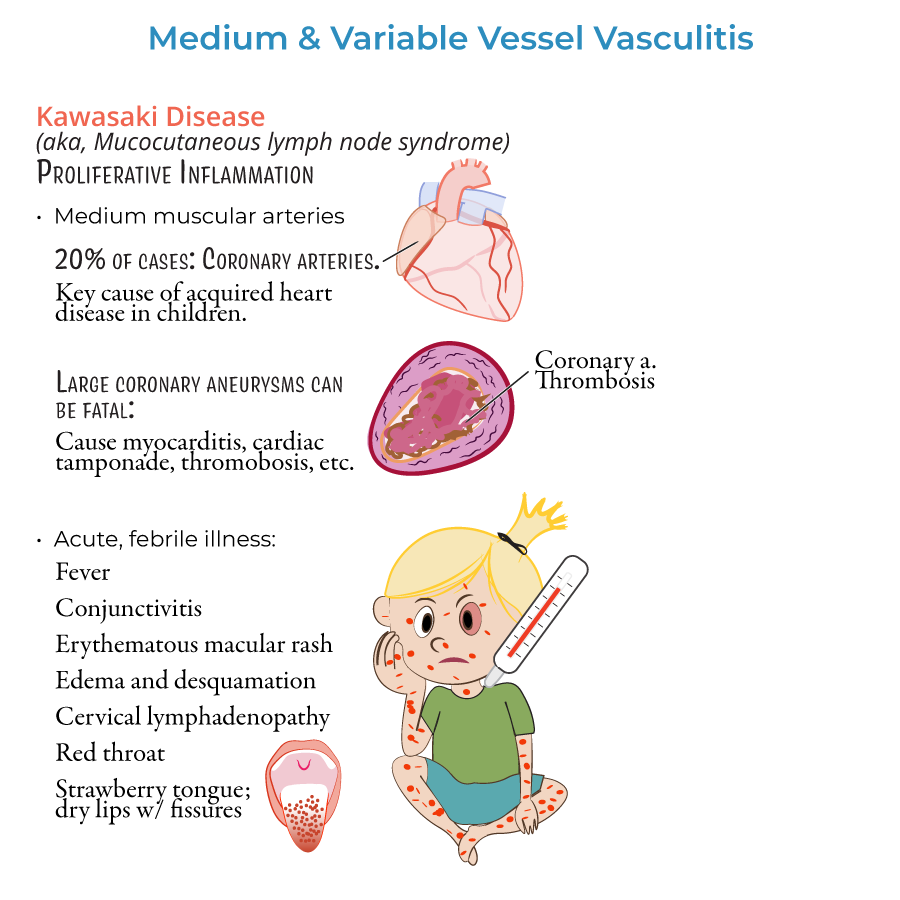
Kawasaki Disease (limited ABIM relevance but tested via coronary pathology)
9. Kawasaki disease is a medium-vessel vasculitis in children, leading to coronary artery aneurysms.
10. Clinical diagnosis:
- Fever ≥5 days plus ≥4 of:
- Conjunctivitis
- Oral mucosal changes (strawberry tongue, cracked lips)
- Extremity changes (edema, desquamation)
- Polymorphous rash
- Cervical lymphadenopathy
- --
HIGH YIELD
Behçet Disease
1. Behçet disease is a vasculitis affecting arteries and veins of all sizes.
2. Clinical features:
- Oral and genital ulcers (painful)
- Uveitis: anterior or posterior
- Skin lesions: erythema nodosum, papulopustular lesions
- Possible vascular thromboses (DVTs, arterial thromboses)
- Clinical diagnosis
- Positive pathergy test (pustule formation after needle stick)
- Corticosteroids for acute flares
- Azathioprine, colchicine, or TNF inhibitors for maintenance.
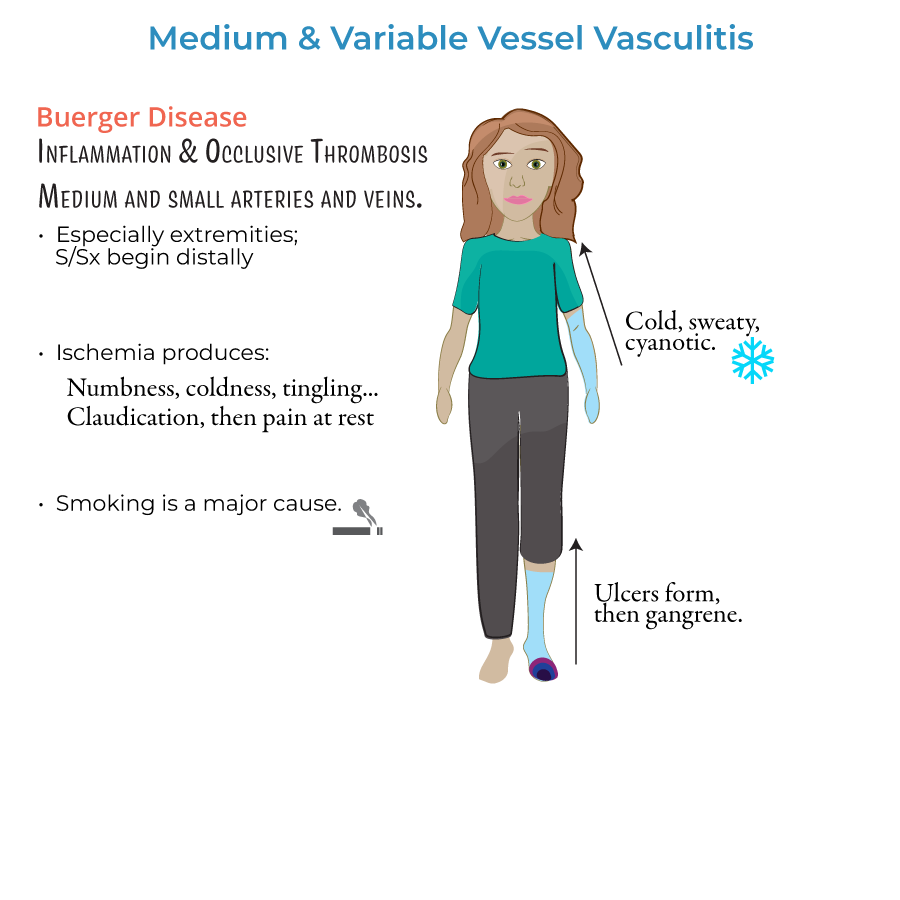
Buerger Disease (Thromboangiitis Obliterans)
6. Buerger disease is a non-atherosclerotic, segmental inflammatory disease affecting small and medium-sized arteries and veins, predominantly in young male smokers.
7. Clinical presentation:
- Distal extremity ischemia
- Claudication progressing to rest pain
- Ulcers, gangrene
- Superficial thrombophlebitis
- Clinical suspicion in young smokers
- Arteriography shows corkscrew collaterals and segmental occlusion.
- Absolute smoking cessation is mandatory; no progression without smoking abstinence.
Histopathology and Imaging Notes
10. PAN: Transmural necrotizing inflammation without granulomas.
11. Kawasaki: Coronary artery inflammation with risk of aneurysmal dilation.
12. Behçet: Neutrophilic vascular infiltration.
13. Buerger: Inflammatory thrombus with sparing of the vessel wall structure.
- --
Beyond the Tutorial
PAN Clinical Management Pearls
1. Pulmonary arteries are spared in PAN (helps distinguish from GPA or MPA).
2. Monitor for complications: mesenteric ischemia, renal infarctions, peripheral neuropathy.
Kawasaki Disease Additional Pearls
3. Post-IVIG, delay live vaccines (MMR, varicella) for 11 months.
4. Children require follow-up echocardiograms to monitor for coronary artery aneurysms.
Behçet Disease Advanced Points
5. Behçet disease increases risk for venous and arterial thrombosis; consider anticoagulation if thrombosis occurs.
6. Retinal vasculitis is a leading cause of vision loss; early ophthalmology involvement is critical.
Buerger Disease Follow-Up
7. Emphasize smoking cessation support programs (pharmacologic aids like varenicline or nicotine replacement).
8. No role for steroids or anticoagulation unless large-vessel thrombosis is present.