
ABIM - Malabsorption Syndromes
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for ABIM from the Malabsorption Syndromes tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
 Below is information not explicitly contained within the tutorial but important for ABIM.
Below is information not explicitly contained within the tutorial but important for ABIM.
- --
VITAL FOR ABIM
Pathophysiology of Malabsorption
1. Malabsorption is the failure to assimilate one or more nutrient types due to defects in digestion, absorption, or transport.
2. Etiologic mechanisms include deficient digestive agents (pancreatic enzymes), abnormal gastrointestinal epithelium, impaired transport, short bowel, and inadequate mixing in the stomach.
3. Clinical presentation includes diarrhea, steatorrhea, weight loss, weakness, anemia, and vitamin/mineral deficiencies.
4. Complications include musculoskeletal abnormalities, neurologic dysfunction (peripheral neuropathy from B vitamin deficiencies), cardiac manifestations, night blindness (vitamin A deficiency), and edema (protein deficiency).
Exocrine Pancreatic Insufficiency (EPI)
1. Occurs when >90% of pancreatic enzyme function is lost, causing malabsorption of fats and fat-soluble vitamins (A, D, E, K, and B12).
2. Primary etiologies include pancreatitis (often alcohol-related in adults), cystic fibrosis (most common pediatric cause), and obstructive pancreatic tumors.
3. Carbohydrate and protein digestion typically remain intact because amylase and protease are also secreted by salivary glands, stomach, and small intestine.
4. Clinical manifestations include loose, bulky, oily, pale feces that float due to oil content; pancreatitis patients experience left epigastric pain radiating to the back.
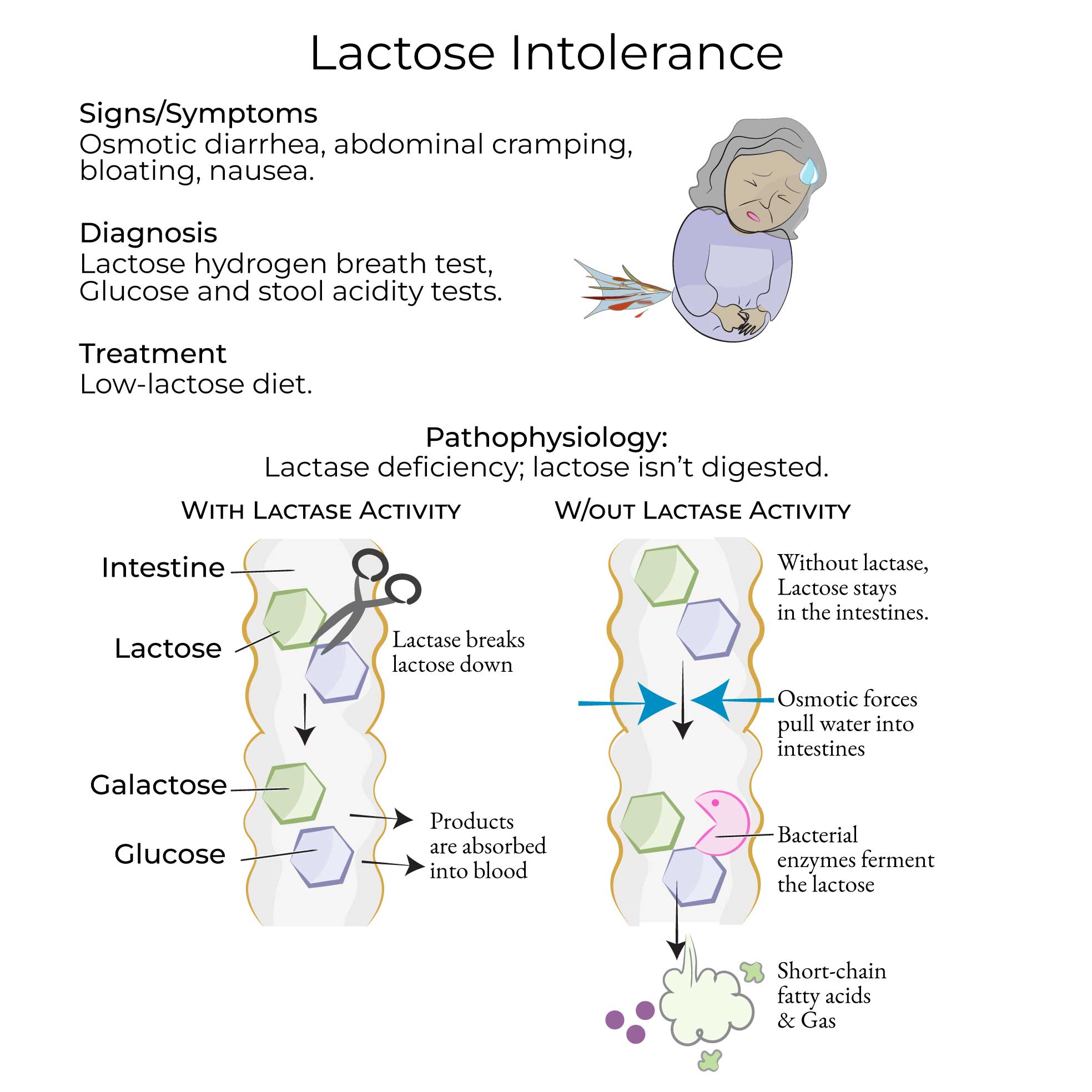
Lactose Intolerance
1. Results from deficient lactase activity with worldwide prevalence >65%, varying significantly by population (30% Europe, 50% US, 70% Asia, nearly 100% Africa).
2. Classified as congenital (rare autosomal recessive), primary (adult-type, common), or secondary (transient due to intestinal damage).
3. Pathophysiology involves osmotic diarrhea from undigested lactose and gas production from bacterial fermentation causing pain, bloating, and flatulence.
4. Diagnosis utilizes hydrogen breath test (>20 ppm increase indicates deficiency), blood glucose tests, DNA tests, and stool acidity tests.
Celiac Disease
1. Autoimmune inflammatory disorder of small bowel triggered by gliadin (in wheat, barley, rye), affecting approximately 1% of US adults.
2. Diagnosis requires serological screening (tTG-IgA, tTG-IgG, deamidated gliadin peptide antibodies, EMA-IgA) followed by endoscopy with small bowel biopsy.
3. Histopathology shows increased lymphocytes, mucosal inflammation, villous atrophy, and crypt hyperplasia upon gluten exposure, which improve with gluten removal.
4. Associated conditions include dermatitis herpetiformis (~10% of patients), reduced bone density, and increased risk of malignancy.
Tropical Sprue
1. Rare disorder occurring in tropical regions (parts of India, Pakistan, Caribbean) with uncertain etiology (likely infectious or environmental).
2. Characterized by malabsorption of folic acid and vitamin B12, leading to megaloblastic anemia.
3. Histopathology reveals villous atrophy, increased crypt depth, epithelial cell enlargement, and lymphocytic/inflammatory cell infiltration.
4. Differentiated from celiac disease through serologic testing despite similar histopathologic features.
Whipple Disease
1. Rare bacterial infection caused by Tropheryma whipplei, predominantly affecting older males of European descent with immune defects.
2. Clinical course typically begins with arthralgias, followed by neurologic symptoms (dementia), endocarditis, and later GI manifestations (diarrhea, abdominal pain, weight loss).
3. Diagnosis requires small bowel biopsy with PAS-positive staining showing foamy macrophages in lamina propria and villous atrophy.
4. PCR testing for T. whipplei DNA in CSF is essential due to potential neurologic complications.
- --
HIGH YIELD
Diagnostic Approach
1. Patient history should focus on stool characteristics, weight loss patterns, and symptom correlation with dietary intake.
2. Blood tests identify specific nutrient deficiencies which may indicate the underlying disorder.
3. Fecal fat tests and Sudan III staining confirm malabsorption, while more directed testing (endoscopy, breath tests, imaging) identifies the cause.
4. Endoscopic findings in celiac disease include duodenal fold "scalloping" and increased vascularity, reflecting villous atrophy and edema.
5. Small bowel biopsy remains the gold standard for diagnosing several malabsorptive disorders, with specific histopathologic features guiding diagnosis.
Management Principles
1. EPI: Treatment includes lifestyle modifications (alcohol cessation), vitamin supplementation, and exogenous pancreatic enzyme administration.
2. Lactose Intolerance: Management involves reducing consumption of lactose-rich foods based on individual tolerance thresholds.
3. Celiac Disease: Strict gluten-free diet is the only effective treatment, with monitoring for adherence and response.
4. Tropical Sprue: Therapy combines folic acid and vitamin B12 supplementation with antibiotics (tetracycline, ampicillin).
5. Whipple Disease: Treatment requires antibiotics (ceftriaxone/penicillin followed by trimethoprim/sulfamethoxazole); fatal if untreated and relapses are common.
Clinical Distinctions
1. Primary vs. secondary lactase deficiency: intestinal villi appear normal in primary but damaged in secondary cases.
2. Lactose intolerance differs from milk allergy, which is an immune-mediated reaction to cow's milk proteins.
3. HLA-DQ2 and HLA-DQ8 testing for celiac disease is primarily useful for ruling out the diagnosis when negative.
4. Chronic pancreatitis can lead to loss of both endocrine and exocrine functions, resulting in diabetes mellitus alongside malabsorption.
5. When tropical sprue and celiac disease have similar histopathology, serologic testing is necessary for differentiation.
- --
Beyond the Tutorial
Advanced Management Considerations
1. Refractory celiac disease: Approach to patients who fail to respond to gluten-free diet.
2. Novel diagnostic biomarkers: Emerging tests to improve diagnostic accuracy and monitoring.
3. Nutritional rehabilitation: Evidence-based protocols for safe refeeding in severely malnourished patients.
4. Malabsorption in inflammatory bowel disease: Mechanisms and management strategies.
5. Bariatric surgery complications: Recognition and management of post-surgical malabsorption.
Preventive and Long-term Care
1. Osteoporosis prevention and treatment in malabsorption disorders.
2. Cancer surveillance recommendations for high-risk malabsorption conditions.
3. Management of extraintestinal manifestations of malabsorption syndromes.
4. Medication absorption issues: Strategies for ensuring therapeutic efficacy in malabsorptive states.
5. Quality of life assessment and improvement in chronic malabsorption disorders.
Special Clinical Scenarios
1. Pregnancy management in women with malabsorption disorders.
2. Elderly patients: Atypical presentations and modified treatment approaches.
3. Multidisciplinary management of complex malabsorption cases.
4. Transitioning adolescents with congenital malabsorption disorders to adult care.
5. Palliative approaches to end-stage disease with malabsorption complications.