
ABIM - ECG
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for ABIM from the Electrocardiogram tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
- --
VITAL FOR ABIM
ECG Fundamentals
1. Records electrical activity of the heart muscle: An ECG reflects and records the electrical activity of the heart muscle.
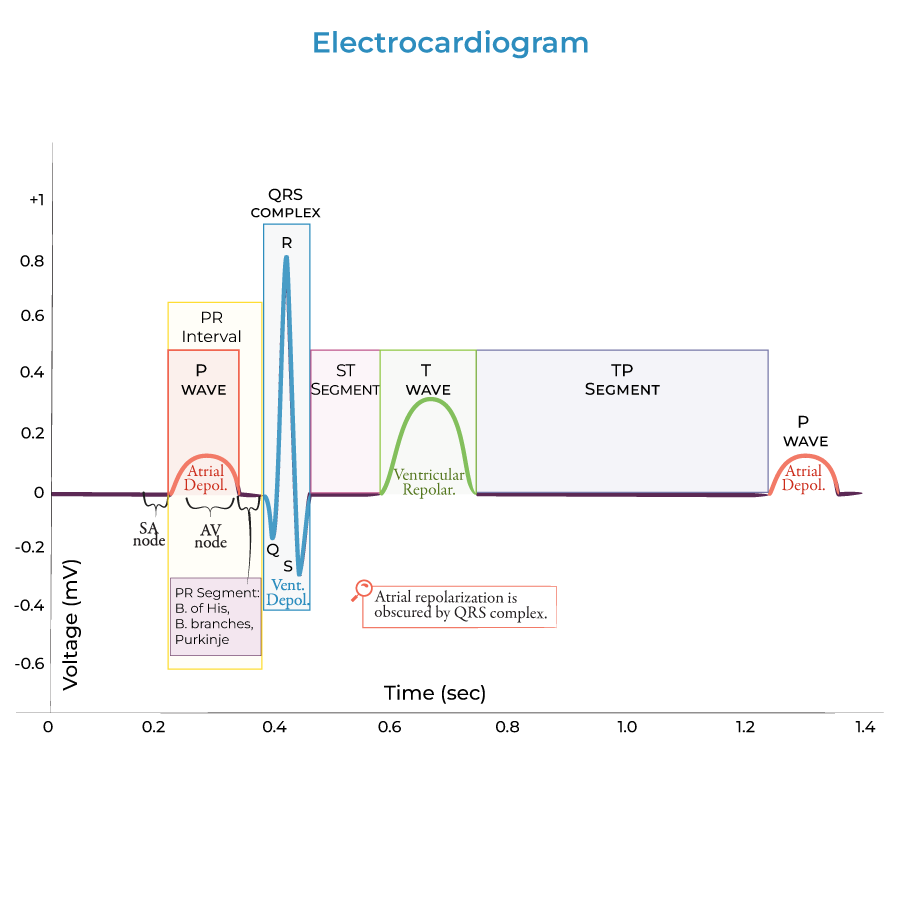
2. Five key waves: A typical ECG comprises 5 waves, labeled P, Q, R, S, and T.
3. Key components include: Waves, which are visible as movement above or below baseline voltage. Segments represent time spent at baseline. Intervals include both segments and waves.
4. Conduction pathway importance: Normal conduction pathway of electrical signals through the heart: SA node → AV node → Bundle of His → Bundle branches → Purkinje fibers.
Critical ECG Interpretations
1. P wave: Reflects the period of atrial depolarization; atrial contraction occurs during the latter part of the P wave.
2. QRS complex: Reflects the period of ventricular depolarization; a wide QRS complex indicates impaired conduction within the ventricles.
3. T wave: Wider and taller than the P wave; reflects the period of ventricular repolarization.
4. PR interval: Begins at the start of the P wave and ends at the start of the QRS complex. PR intervals lasting longer than 0.12 - 0.20 seconds may indicate AV conduction block.
5. ST segment: Begins after the QRS complex and ends at the onset to the T wave. Ventricular contraction begins during the QRS complex and continues through the ST segment.
- --
HIGH YIELD
Electrophysiological Principles
1. Depolarization and repolarization: Depolarization occurs when the membrane potential becomes more positive. Repolarization occurs when the membrane potential returns to negative.
2. Resting potential: Normal resting potential of ventricular cardiac cells is approximately -90 millivolts.
3. Pacemaker function: Sinoatrial (SA) node is the pacemaker of the heart; it sets the heart's rhythm. It sends electrical signals throughout the atria, and to the atrioventricular (AV) node.
4. Ventricular activation sequence: This arrangement ensures that ventricular depolarization and subsequent contraction begins at the apex and moves towards the atria; this pathway moves blood out of the ventricles.
Clinical Correlations
1. U wave findings: A prominent U wave may reflect bradycardia (slow heart rate), hypokalemia, ischemia, or effects of antiarrhythmic drugs.
2. Heart rate calculation: Calculate the PP interval, which is the distance between P waves of successive cardiac cycles, or the RR interval, which is the distance between successive R waves.
3. Bundle branch block: A wide QRS complex indicates impaired conduction within the ventricles, as in bundle branch block.
4. PR segment significance: Within the PR interval, the AV node fires, sending the electrical signal through the bundle of His, bundle branches, and to the Purkinje fibers.
- --
Beyond the Tutorial
Advanced ECG Interpretation
1. Wave morphology interpretation: Unlike in action potential graphs, the shape of the wave does not indicate depolarization or repolarization – both the P wave and T wave are positive, but the P wave reflects depolarization and the T wave reflects repolarization.
2. Lead positioning: The ECG only shows the direction of current flow relative to the lead's axis.
3. Mechanical-electrical correlation: Isovolumetric contraction begins during the QRS complex, and the ST segment reflects the period of ventricular ejection of blood into the great vessels.
4. Pathological patterns: The tutorial mentions AV conduction block, but internists should recognize specific patterns of various degrees of block and other arrhythmias.
5. Effect of electrolyte abnormalities: While hypokalemia is mentioned with U waves, other electrolyte abnormalities have characteristic ECG findings not explicitly detailed.
6. QRS obscuration: The QRS complex masks the atrial repolarization wave which would otherwise be visible.