
ABIM - Diabetes Mellitus Pathophysiology
Start your One-Week Free Trial
Already subscribed? Log in »
Here are key facts for American Board of Internal Medicine (ABIM) Exam from the Diabetes Mellitus - Pathophysiology tutorial, as well as points of interest at the end of this document that are not directly addressed in this tutorial but should help you prepare for the boards. See the tutorial notes for further details and relevant links.
 2. Type 1 vs. Type 2 presentation:
Below is information not explicitly contained within the tutorial but important for the ABIM Exam.
2. Type 1 vs. Type 2 presentation:
Below is information not explicitly contained within the tutorial but important for the ABIM Exam.
- --
VITAL FOR ABIM EXAM
Diabetes Mellitus - Diagnosis & Classification
1. Diagnostic criteria: Random plasma glucose level of 200+ mg/dL or a fasting plasma glucose level of 126+ mg/dL.
2. Pathophysiologic consequence: Chronic hyperglycemia produces dysfunction and damage of multiple organs, including the heart, kidneys, eyes, and peripheral nervous system.
3. Classification: Type 1, Type 2, Monogenic diabetes (including MODY), Secondary diabetes, and Gestational diabetes.
4. Prediabetes recognition: Condition where glucose levels are elevated, but not high enough to be classified as diabetes; patients are at high risk for Type 2 diabetes and cardiovascular complications.
Type 1 Diabetes - Clinical Approach
1. Epidemiology: Accounts for 5-10% of all diabetes mellitus cases.
2. Pathophysiology: Caused by autoimmune destruction of pancreatic beta cells; insulitis often visible in pancreatic tissue samples.
3. Immunological markers: Islet autoantibodies including those targeting insulin, GAD65, ZnT8, and IA2.
4. Genetic associations: Variations in HLA alleles, particularly class II DR and DQ cell-surface proteins.
5. Treatment principle: Requires exogenous insulin administration due to absolute insulin deficiency.
Type 2 Diabetes - Clinical Approach
1. Epidemiology: Represents 90-95% of all diabetes cases.
2. Pathophysiology: Characterized by peripheral tissue insulin resistance and relative insulin deficiency due to mild beta cell destruction caused by amyloid deposits.
3. Risk factors: Associated with obesity, central fat distribution, sedentarism, stress, and inflammation.
4. Treatment approach: Treatment is complex and needs to be tailored to the individual and achievable glycemic targets.
5. Management algorithm:
- First line: Diet and exercise, and perhaps administration of Metformin, which decreases hepatic glucose production
- Second line: Insulin, GLP-1 receptor agonists, or SGLT2-inhibitors if hyperglycemia persists
Acute Complications - Management
1. Diabetic Ketoacidosis (DKA):
- Association: Occurs in under-treated Type 1 diabetes
- Clinical presentation: Nausea and vomiting, fatigue, "fruity" odor, and Kussmal breathing
- Pathophysiology: Reflects the acidic state of the body, can lead to coma
- Management: Fluids, electrolytes, and insulin to normalize blood glucose
- Association: More common in Type 2 diabetes
- Pathophysiology: Occurs when a patient with polyuria has deficient water intake leading to severe dehydration
- High-risk groups: Patients unable to drink on their own, such as after a stroke or other debilitating conditions
- Mortality risk: Has a mortality rate of up to 20% - much higher than diabetic ketoacidosis
- Management: Requires saline, insulin, and electrolytes
- --
HIGH YIELD
Clinical Presentation & Diagnosis
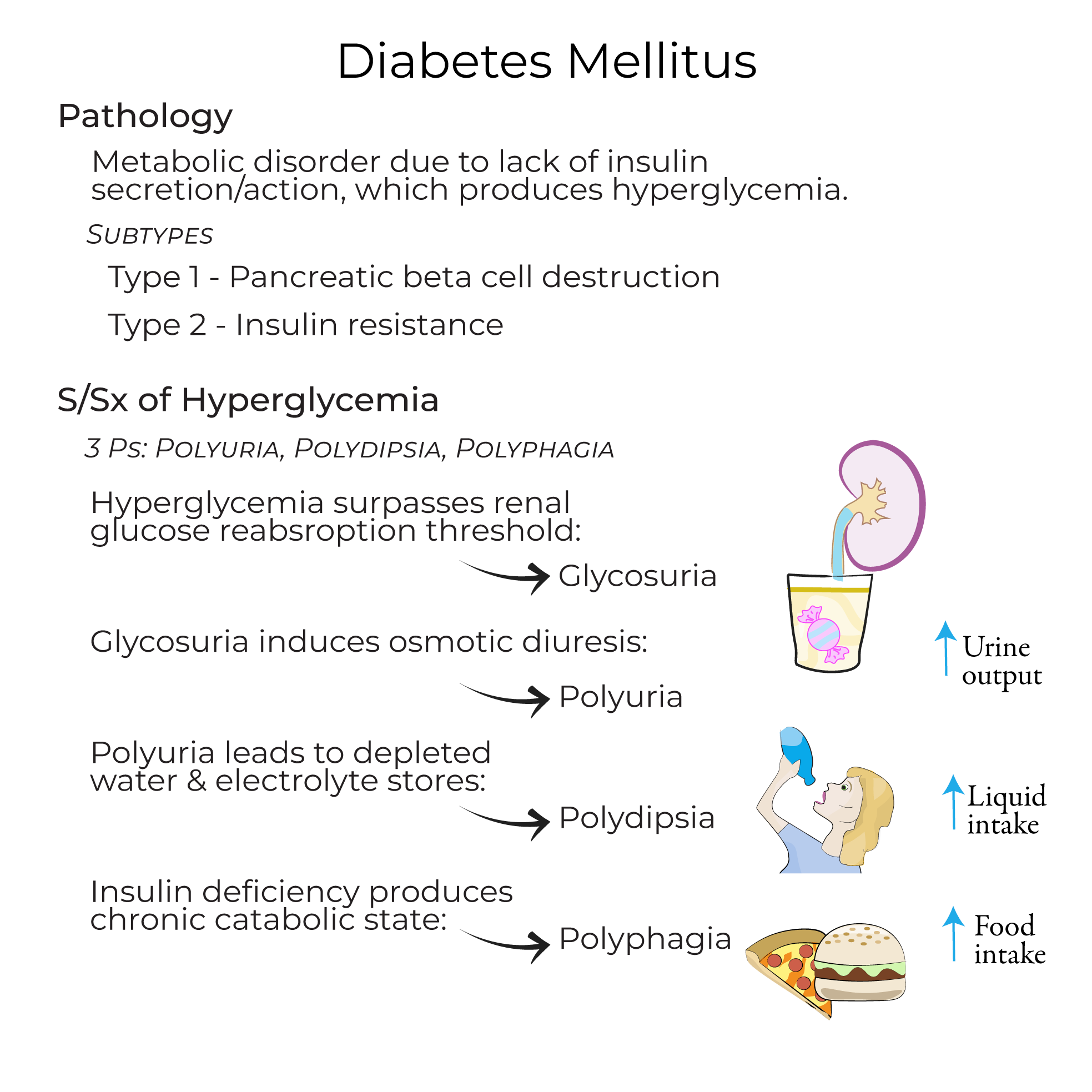
1. Classic triad (the "3 P's"):
- Polyuria: Glycosuria induces osmotic diuresis
- Polydipsia: Results from depleted water and electrolyte stores
- Polyphagia: Caused by chronic catabolic state
2. Type 1 vs. Type 2 presentation:
- Type 1: Often symptomatic at presentation with progressive insulin deficiency
- Type 2: Many patients are asymptomatic with diagnosis occurring after routine blood testing
- Type 1 in adults: Some adults diagnosed with Type 2 diabetes based upon age may be misclassified, which can have deleterious effects on their treatment
- Type 2 in children: Historically adult-onset but increasingly common in children due to higher rates of childhood obesity and inactivity
Therapeutic Considerations
1. Type 1 insulin management:
- Clinical course: Shows progressive reduction in insulin levels as more cells are destroyed
- Variability: Hyperglycemia may be transient in some cases, with variable insulin needs, particularly in adults
- Variant awareness: Idiopathic Type 1 diabetes exists without autoimmune involvement, though very rare
- Insulin dynamics: Patients may initially have elevated insulin levels in response to insulin resistance; levels eventually fall as pancreatic cells can't sustain production
- Exercise benefit: Increases Glut-4 receptors in skeletal muscle, improving insulin sensitivity
- Medication considerations: Drugs can be costly and/or have contraindications that must be considered for each patient
- Treatment goal: Reach glycemic targets to avoid organ damage caused by hyperglycemia
Chronic Complications - Prevention & Management
1. Vascular disease:
- Pathogenesis: Results from chronic hyperglycemia
- Manifestations: Can lead to heart failure and atherosclerosis (which can produce myocardial infarction or stroke), kidney damage, visual impairment, and peripheral nerve dysfunction
- Growth concerns: Impaired growth in children
- Infection risk: Increased susceptibility to infection due to immune suppression
- Iatrogenic complication: Hypoglycemia due to missing a meal, excessive physical exertion, or excessive insulin administration
- --
Beyond the Tutorial
Evidence-Based Management
1. Glycemic targets: Individualizing HbA1c goals based on age, comorbidities, life expectancy, and hypoglycemia risk.
2. Cardiovascular risk reduction: ASCVD risk assessment and management in patients with diabetes.
3. Medication selection: Comparative effectiveness and safety of newer diabetes medications.
Special Clinical Scenarios
1. Hospital management: Inpatient glycemic targets and insulin protocols for critically and non-critically ill patients.
2. Perioperative care: Management of diabetes medications during the perioperative period.
3. Steroid-induced hyperglycemia: Approach to diagnosis and management.
Complication Screening & Management
1. Microvascular complications: Evidence-based approaches to screening, prevention, and management of retinopathy, nephropathy, and neuropathy.
2. Diabetic kidney disease: Role of SGLT2 inhibitors, GLP-1 RAs, and ACE/ARBs in prevention and management.
3. Diabetic foot care: Comprehensive assessment, prevention strategies, and management of diabetic foot ulcers.
Technology in Diabetes Care
1. Continuous glucose monitoring: Indications, interpretation of data, and impact on management decisions.
2. Insulin delivery devices: Selection and use of insulin pumps and artificial pancreas systems.
3. Telemedicine: Implementation and effectiveness in diabetes management.