

Start your One-Week Free Trial
Already subscribed? Log in »
Uterus & Uterine Tubes
Here we’ll learn the anatomy of the uterus and uterine tubes, which undergo histological changes in response to ovarian hormones throughout the menstrual cycle.
 Aka fallopian tubes
Aka fallopian tubes
 The uterine cavity is the inverted triangular space inside the uterus; during pregnancy, the growing fetus fills and expands this space.
The uterine horns are continuous with the uterine tubes.
The uterine cavity is the inverted triangular space inside the uterus; during pregnancy, the growing fetus fills and expands this space.
The uterine horns are continuous with the uterine tubes.
 The most common forms cervical cancer can be prevented by HPV vaccines, which are caused by the Human Papilloma Viruses types 16 and 18. The availability of HPV vaccines and cancer screening with Pap smear tests have reduced the rates of cervical cancer incidence and mortality in the US and other wealthy countries. You can learn more about cervical cancer in our notes.
Pelvic inflammatory disease (PID) occurs when untreated sexually transmitted infections spread from the vagina to the uterus, uterine tubes, or ovaries. Chlamydia and gonorrhea are the most common causes of PID, which causes pain, fever, vaginal discharge, and long, heavy periods; long-term complications include infertility.
Ectopic Pregnancy
Additional Non-Neoplasm Pathologies:
Cervical pathologies
Embryology Overview
The most common forms cervical cancer can be prevented by HPV vaccines, which are caused by the Human Papilloma Viruses types 16 and 18. The availability of HPV vaccines and cancer screening with Pap smear tests have reduced the rates of cervical cancer incidence and mortality in the US and other wealthy countries. You can learn more about cervical cancer in our notes.
Pelvic inflammatory disease (PID) occurs when untreated sexually transmitted infections spread from the vagina to the uterus, uterine tubes, or ovaries. Chlamydia and gonorrhea are the most common causes of PID, which causes pain, fever, vaginal discharge, and long, heavy periods; long-term complications include infertility.
Ectopic Pregnancy
Additional Non-Neoplasm Pathologies:
Cervical pathologies
Embryology Overview
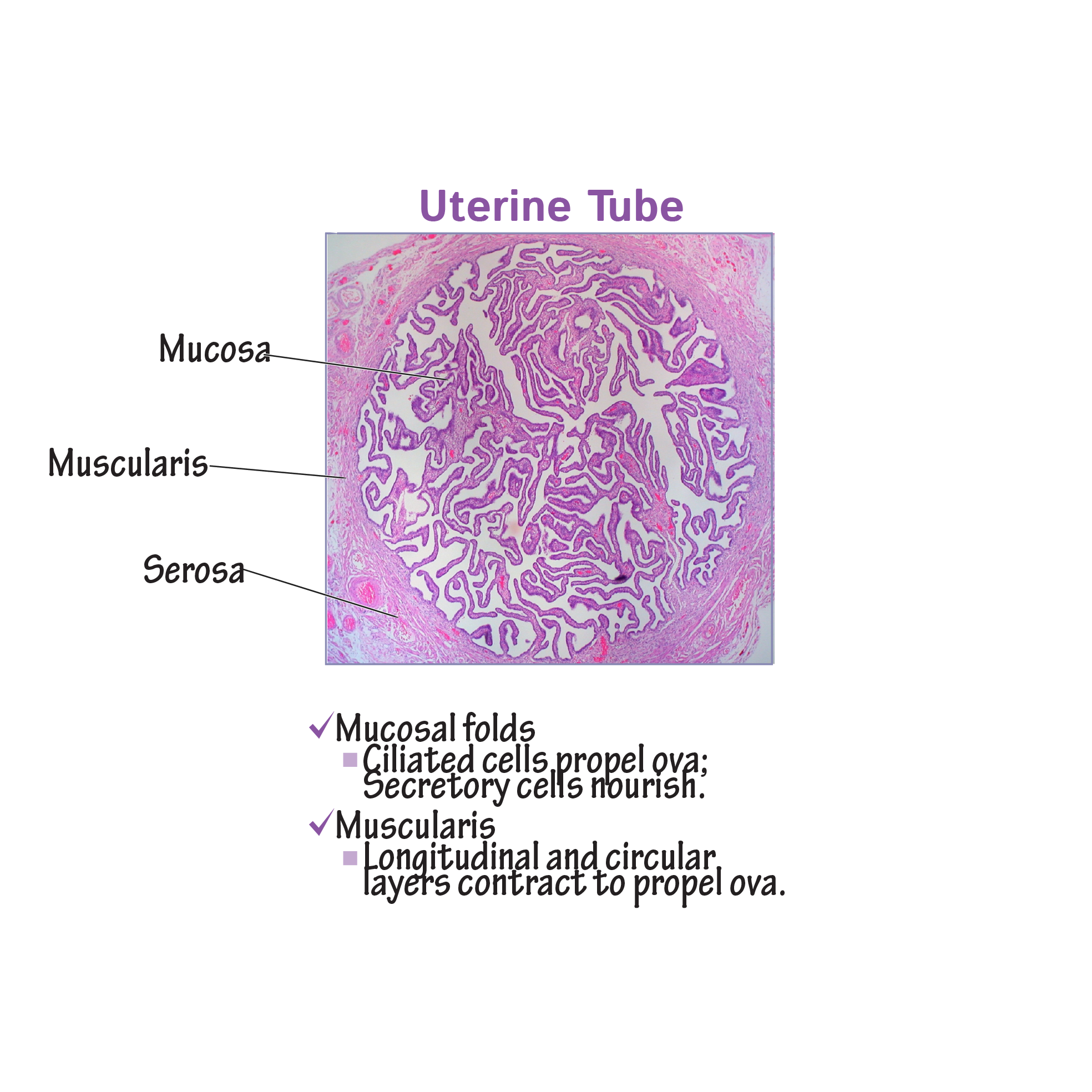
Uterine tubes
Three tunics:
The inner mucosa comprises longitudinal folds covered by ciliated epithelium and non-ciliated secretory cells. The ciliated cells help “sweep” ova towards the uterus. Secretions from uterine tube cells provide nutrition for the ova and aids in capacitation of sperm cells, which is necessary for fertilization.
The muscularis layer comprises an inner circular and an outer longitudinal layer; the muscularis produces peristaltic contractions that move the ova towards the uterus.
The outermost layer is the serosa.
4 segments:
The intramural (aka uterine) segment arises within the muscular wall of the uterus; this segment regulates the passage of sperm and other materials into the uterine tubes.
The isthmus is the next segment; it comprises a relatively thick muscularis layer; sperm are temporarily held, waiting for uterine tube secretions to stimulate capacitation.
The ampulla is the thinner-walled dilated portion of the uterine tube; this is the most common site of fertilization (joining of the ovum and sperm to create a zygote).
The infundibulum is the wide funnel-shaped lateral end of the uterine tube.
Indicate that fimbriae are the finger-like projections of the infundibulum; the singular ovarian fimbria is the only direct attachment between the uterine tube and ovary.
The abdominal ostium is where the uterine tube opens to the abdominal cavity. When ova are released from the ovaries, they move into the abdominal ostium and are “ushered” into the uterine tube by the fimbriae.
Uterus
Three tunics of the uterus
Continuous with those of the uterine tubes
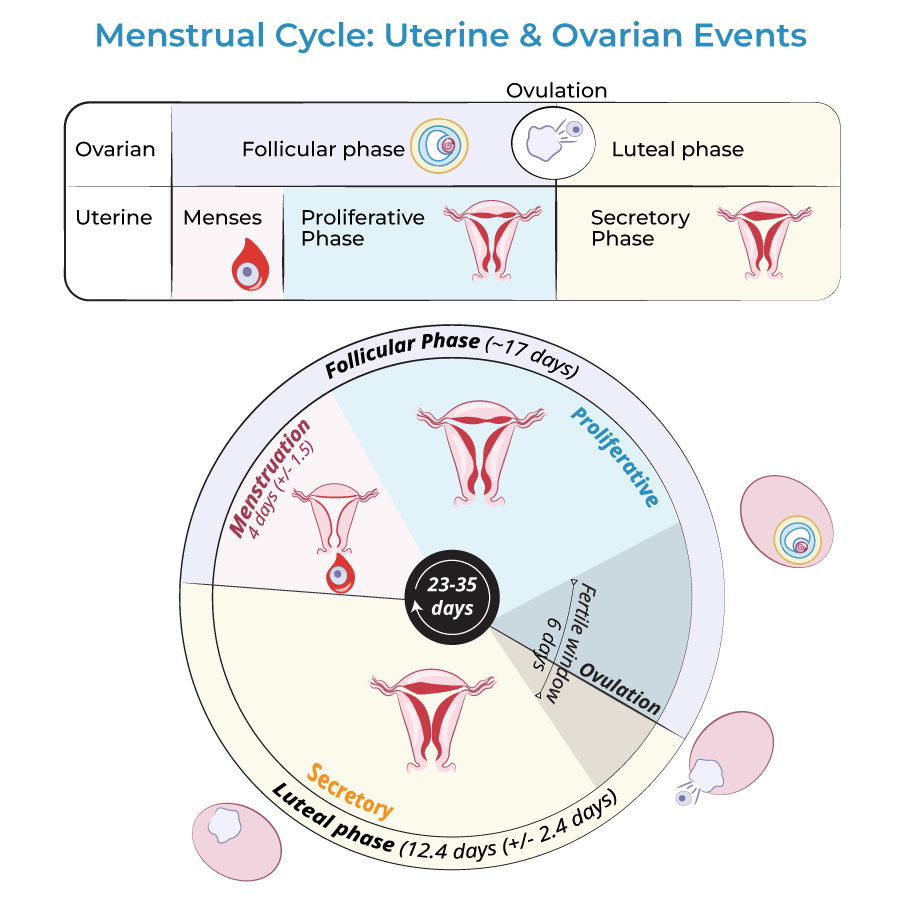
The endometrium is the dynamic innermost layer that builds up and sheds over the course of a menstrual cycle; growth of the endometrium is under direction of the ovarian hormones estrogen and progesterone.
During menses, the outermost layer, called the functional layer, is shed and expelled along with the oocyte. The onset of menses (aka menstruation) marks the onset of the menstrual cycle.
During the proliferation phase of the cycle, estrogen induces endometrial re-growth.
After ovulation, which is when the ovum is released from the oocyte, the secretory phase begins and rising progesterone levels induce the growth of glandular and vascularized tissue in the endometrium.
The secretory phase prepares the endometrium for potential implantation of a fertilized ovum; if implantation is successful, menstruation does not occur and the early placenta begins to form.
In the absence of successful implantation, menses occurs and the cycle starts again.
Menstrual Cycle
The myometrium is a thick layer of interweaving bundles of smooth muscle tissue that contracts during orgasm, childbirth, and menstruation under the influence of oxytocin and prostaglandins.
The perimetrium is the serosal covering of the uterus.
Regions of the uterus:
The fundus is the uppermost portion of the uterus; it is above the uterine tubes.
The body is the largest portion of the uterus; it is also referred to as the corpus.
The isthmus is the region of the uterus that constricts just before the cervix, which is the most inferior portion of the uterus; the cervix is continuous with the vagina.
The internal os is the opening between the isthmus and the cervix; the external os is the opening between the cervix and vagina. Recall that this portion of the cervix projects into the upper vagina.
The spindle-shaped cervical canal is between the internal os and external os. Glands within the cervical canal secrete the mucus that either block or facilitate the entry of sperm into the uterus, depending on the time of the menstrual cycle (see our notes for more information).
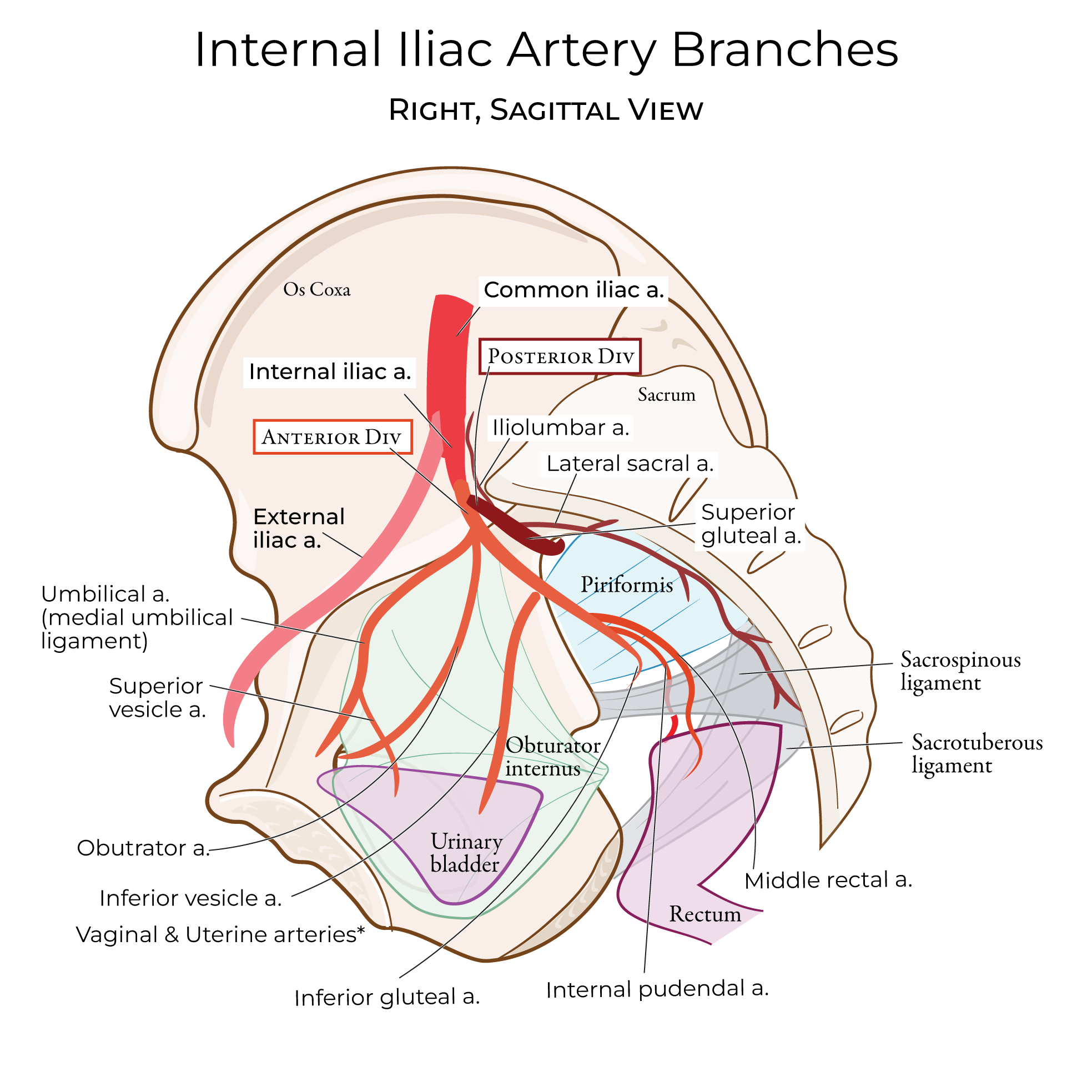
Blood supply and innervation
Arterial blood is supplied to the uterus and uterine tubes via the uterine and ovarian arteries; venous drainage is via the uterine venous plexus. Innervation is provided by the inferior hypogastric plexus.
Clinical Correlations
Embryology Overview