

Start your One-Week Free Trial
Already subscribed? Log in »


Vulva and Superficial Perineal Pouch
Here we’ll learn the anatomy of the vulva and the superficial perineal pouch.
The vulva refers to the typical female genitalia; it comprises structures that are sexually responsive and/or protect the vaginal opening.
We show the vaginal orifice (the opening of the vagina).
Around the edges of the orifice, weshow the hymen caruncles, which are remnants of the hymen.
At birth, the hymen partially closes the vaginal orifice, and over time is stretched and/or torn by physical activity, tampon use, and sexual intercourse. In a condition called imperforate hymen, the membrane completely closes off the opening to the vagina, resulting in the accumulation of uterovaginal secretions and menstrual blood, which can cause pain.
The ducts of the greater vestibular glands are posterolateral to the vaginal orifice; they release lubricating mucus upon sexual arousal.
The external urethral orifice and the nearby ducts of the paraurethral glands are anterior to the vaginal orifice. The paraurethral ducts vary in number (these are also referred to as Skene’s glands and lesser vestibular glands). The paraurethral gland secretions are thought to lubricate the vestibule of the vagina and have antimicrobial properties.
The glans of the clitoris is the portion of the clitoris that is externally visible and highly sensitive, with approximately 10,000 nerve endings.
The labia minora have medial and lateral folds; they comprise erectile tissues rich in vasculature.
The right and left medial folds meet anteriorly to form the frenulum of the clitoris; the right and left lateral folds meet at the prepuce (aka hood) of the clitoris, which covers the glans of the clitoris.
Posteriorly, the folds merge to form the frenulum of the labia minora (aka fourchette).
The area between the labia minora is the vestibule of the vagina.
The labia majora comprise adipose and smooth muscle tissue covered in skin, and, post-puberty, with hair.
Where the labia majora meet anteriorly they form the mons pubis; this is the mound of fatty tissue superficial to the pubic symphysis.
Posteriorly, the labia majora meet at the posterior commissure, which overlies the perineal body. The perineal body is a fibromuscular structure at the junction of the anus and urogenital triangle that strengthens the pelvic floor and provides attachment for pelvic floor and perineal muscles.
Next let’s learn about the perineal compartment, which is subdivided into deep and superficial pouches by the perineal membrane, regardless of sex.
The superficial perineal pouch is the potential space between the superficial perineal fascia and the perineal membrane. It contains the erectile tissues and overlying muscles.
In contrast, the deep perineal pouch is between the inferior fascia of the pelvic diaphragm and the perineal membrane. It contains the urethra, vagina (when present), the deep transverse perineal and sphincter urethral muscles, the bulbourethral gland (when present) and the pudendal artery and nerve branches (which supply the clitoris or penis).
We draw the superficial perineal pouch, which we’ll further subdivide into superficial and deeper structures.
The pubic rami of the pelvis in inferior view provide an anchor for the soft tissues of the urogenital triangle, which is the anterior portion of the perineum (the posterior portion is the anal triangle, you can learn more about this in our notes).
The perineal membrane has openings for the vagina and urethra to pass.
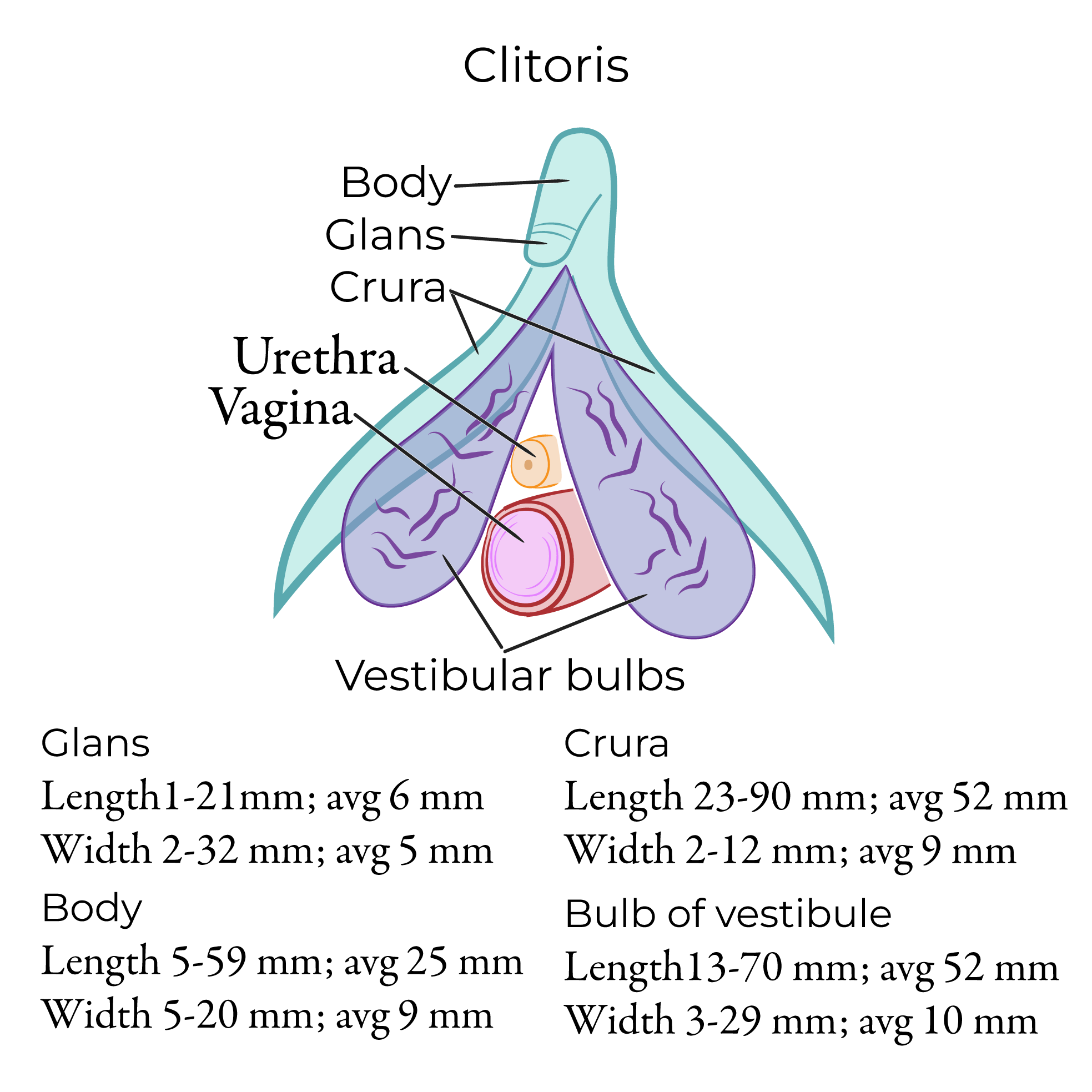
The clitoris:
The glans is the sensitive external portion that we drew in our prior diagram.
The paired corpus cavernosa are the erectile bodies of the clitoris; we’re only seeing part of them, here.
The body is the “free portion” where the corpus cavernosa meet medially, and the crura are the “legs” of the clitoris that extend laterally and attach to the pubic rami and perineal membrane.
The suspensory ligament, which anchors the clitoris to the pubic symphysis and pubic arch.
The vestibular bulbs (bulbs of the vestibule) lie lateral to the opening of the vagina, deep to the labia minora. The vestibular bulbs are erectile tissues that are closely associated with the glans of the clitoris; because of their relationship to the clitoris and their role in sexual pleasure, they are sometimes referred to as the bulbs of the clitoris.
 Posterior to the vestibular bulbs, we see the pea-sized greater vestibular glands (aka Bartholin’s glands). The vestibular glands release lubricating secretions during sexual arousal; we drew the openings of their ducts in our previous diagram.
Cysts can form when the greater vestibular gland ducts become obstructed and secretions accumulate. These cysts are usually asymptomatic and resolve on their own, but they can become infected and form painful abscesses.
Next, on the superficial side of our diagram, we show the muscles that overlie the erectile tissues:
The ischiocavernosus muscle covers the crura of the clitoris.
The bulbospongiosus muscle covers the vestibular bulbs and the greater vestibular gland.
Some of the fibers of bulbospongiosus blend with those of ischiocavernosus, while others travel further and arch over the body of the clitoris.
These muscles compress the corpus cavernosa of the clitoris during sexual arousal, maintaining increased blood pressure in the erectile tissue.
For completeness, show that the superficial transverse perineal muscles arise from the ischial bones and meet at the perineal body, which they help to stabilize.
Arterial blood supply to the perineum is via primarily the internal pudendal artery, which is a branch of the internal iliac artery; the labia majora also receive blood from the superficial external pudendal artery, which is a branch of the femoral artery.
Venous drainage is via the internal pudendal vein, which drains into the internal iliac vein, and the external pudendal vein, which drains into the great saphenous vein.
Motor and sensory innervation is via the pudendal nerve (S2-S4 spinal roots), which splits into the dorsal nerve of the clitoris, perineal nerve, and inferior rectal nerve. Sympathetic innervation of the external genitalia arises from T11-L2 (via the hypogastric plexus), parasympathetic innervation arises from S2-S4 (via pelvic splanchnic nerves).
Vaginitis refers to infection and inflammation of the vagina and vulva. Vaginitis is a common condition most often caused by bacteria. On a wet mount, we’ll see clue cells, which are vaginal epithelial cells studded with bacteria, which can give the cells a “fuzzy” appearance. Candida infection, aka yeast infection, is another common cause of vaginitis.
Episiotomy is an incision through the perineum to widen the vaginal opening for childbirth. This procedure was routine from the 1940s through the 1980s, but studies show that episiotomies increase the risk of blood loss, infection, and pain, and alternative methods to assist in perineal stretches are often preferred. Episiotomies are still often recommended in cases of fetal distress to speed up delivery.
Additional vaginal/vulvar pathologies
Clitoris measurements: https://onlinelibrary.wiley.com/doi/10.1002/ca.24113
Posterior to the vestibular bulbs, we see the pea-sized greater vestibular glands (aka Bartholin’s glands). The vestibular glands release lubricating secretions during sexual arousal; we drew the openings of their ducts in our previous diagram.
Cysts can form when the greater vestibular gland ducts become obstructed and secretions accumulate. These cysts are usually asymptomatic and resolve on their own, but they can become infected and form painful abscesses.
Next, on the superficial side of our diagram, we show the muscles that overlie the erectile tissues:
The ischiocavernosus muscle covers the crura of the clitoris.
The bulbospongiosus muscle covers the vestibular bulbs and the greater vestibular gland.
Some of the fibers of bulbospongiosus blend with those of ischiocavernosus, while others travel further and arch over the body of the clitoris.
These muscles compress the corpus cavernosa of the clitoris during sexual arousal, maintaining increased blood pressure in the erectile tissue.
For completeness, show that the superficial transverse perineal muscles arise from the ischial bones and meet at the perineal body, which they help to stabilize.
Arterial blood supply to the perineum is via primarily the internal pudendal artery, which is a branch of the internal iliac artery; the labia majora also receive blood from the superficial external pudendal artery, which is a branch of the femoral artery.
Venous drainage is via the internal pudendal vein, which drains into the internal iliac vein, and the external pudendal vein, which drains into the great saphenous vein.
Motor and sensory innervation is via the pudendal nerve (S2-S4 spinal roots), which splits into the dorsal nerve of the clitoris, perineal nerve, and inferior rectal nerve. Sympathetic innervation of the external genitalia arises from T11-L2 (via the hypogastric plexus), parasympathetic innervation arises from S2-S4 (via pelvic splanchnic nerves).
Vaginitis refers to infection and inflammation of the vagina and vulva. Vaginitis is a common condition most often caused by bacteria. On a wet mount, we’ll see clue cells, which are vaginal epithelial cells studded with bacteria, which can give the cells a “fuzzy” appearance. Candida infection, aka yeast infection, is another common cause of vaginitis.
Episiotomy is an incision through the perineum to widen the vaginal opening for childbirth. This procedure was routine from the 1940s through the 1980s, but studies show that episiotomies increase the risk of blood loss, infection, and pain, and alternative methods to assist in perineal stretches are often preferred. Episiotomies are still often recommended in cases of fetal distress to speed up delivery.
Additional vaginal/vulvar pathologies
Clitoris measurements: https://onlinelibrary.wiley.com/doi/10.1002/ca.24113
Vulva/External Genitalia
Perineal Pouches
Posterior to the vestibular bulbs, we see the pea-sized greater vestibular glands (aka Bartholin’s glands). The vestibular glands release lubricating secretions during sexual arousal; we drew the openings of their ducts in our previous diagram.
Cysts can form when the greater vestibular gland ducts become obstructed and secretions accumulate. These cysts are usually asymptomatic and resolve on their own, but they can become infected and form painful abscesses.
Next, on the superficial side of our diagram, we show the muscles that overlie the erectile tissues:
The ischiocavernosus muscle covers the crura of the clitoris.
The bulbospongiosus muscle covers the vestibular bulbs and the greater vestibular gland.
Some of the fibers of bulbospongiosus blend with those of ischiocavernosus, while others travel further and arch over the body of the clitoris.
These muscles compress the corpus cavernosa of the clitoris during sexual arousal, maintaining increased blood pressure in the erectile tissue.
For completeness, show that the superficial transverse perineal muscles arise from the ischial bones and meet at the perineal body, which they help to stabilize.
Arterial blood supply to the perineum is via primarily the internal pudendal artery, which is a branch of the internal iliac artery; the labia majora also receive blood from the superficial external pudendal artery, which is a branch of the femoral artery.
Venous drainage is via the internal pudendal vein, which drains into the internal iliac vein, and the external pudendal vein, which drains into the great saphenous vein.
Motor and sensory innervation is via the pudendal nerve (S2-S4 spinal roots), which splits into the dorsal nerve of the clitoris, perineal nerve, and inferior rectal nerve. Sympathetic innervation of the external genitalia arises from T11-L2 (via the hypogastric plexus), parasympathetic innervation arises from S2-S4 (via pelvic splanchnic nerves).
Clinical Correlations