

Start your One-Week Free Trial
Already subscribed? Log in »
Elbow Joint
Here we'll learn about the joints of the elbow.
The elbow comprises two hinge joints that function together:
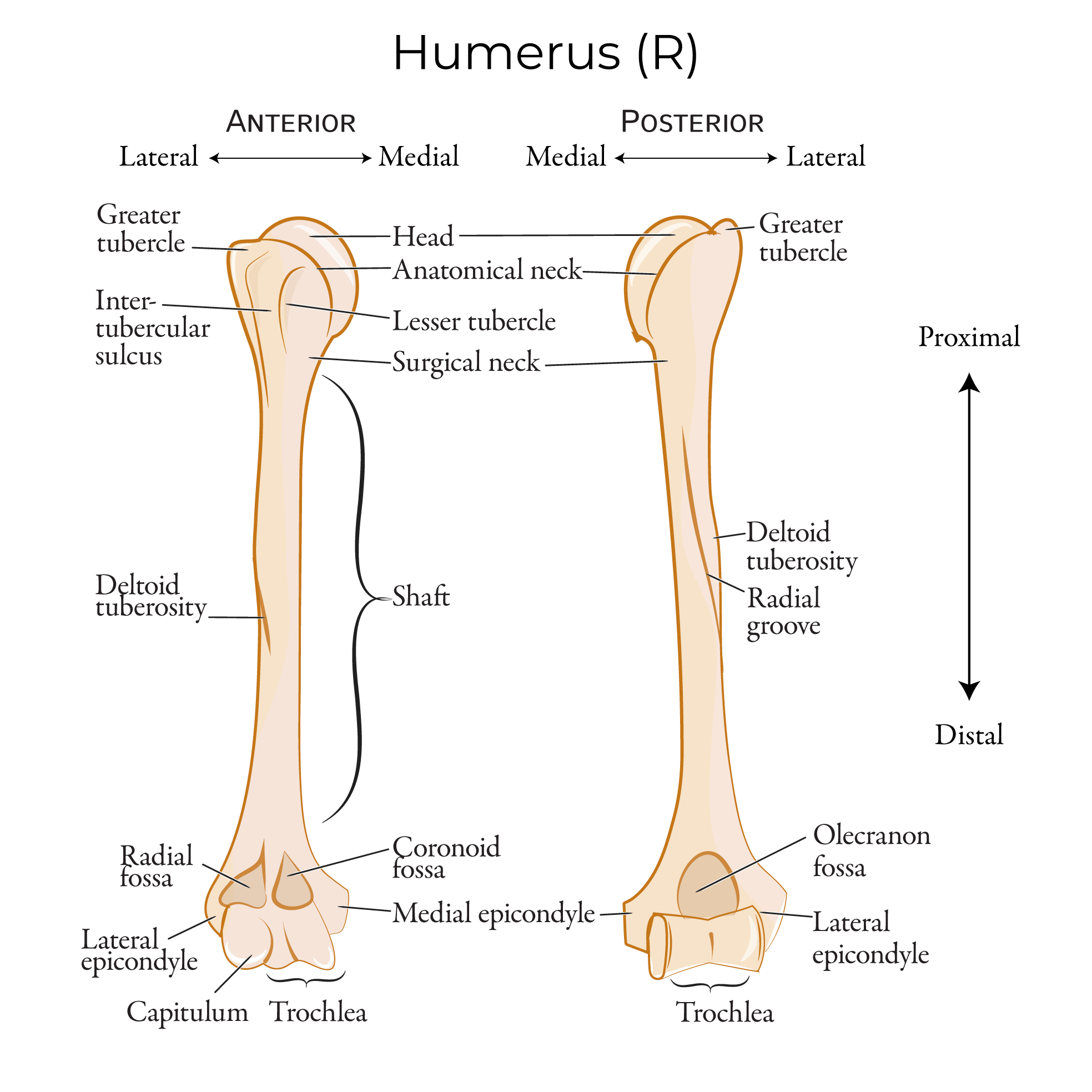
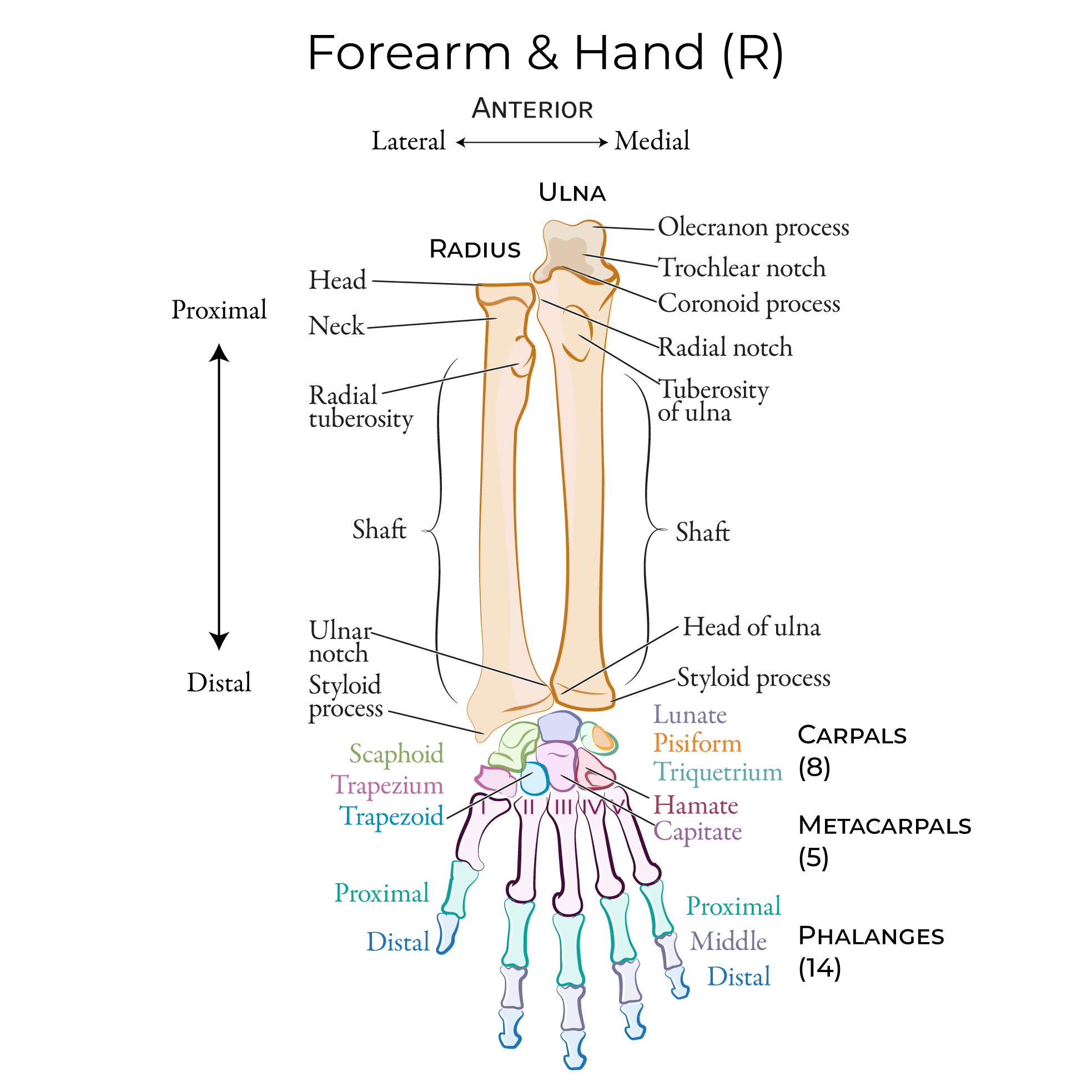
The trochlea of the humerus articulates with the trochlear notch of the ulna.
The capitulum of the humerus articulates with the head of the radius.
Together, these articulations comprise a synovial hinge joint capable of extension and flexion of the forearm.
The proximal radio-ulnar joint is formed by the articulation between the head of the radius and the radial notch of the ulna; this is a pivot joint that allows for forearm supination and pronation.
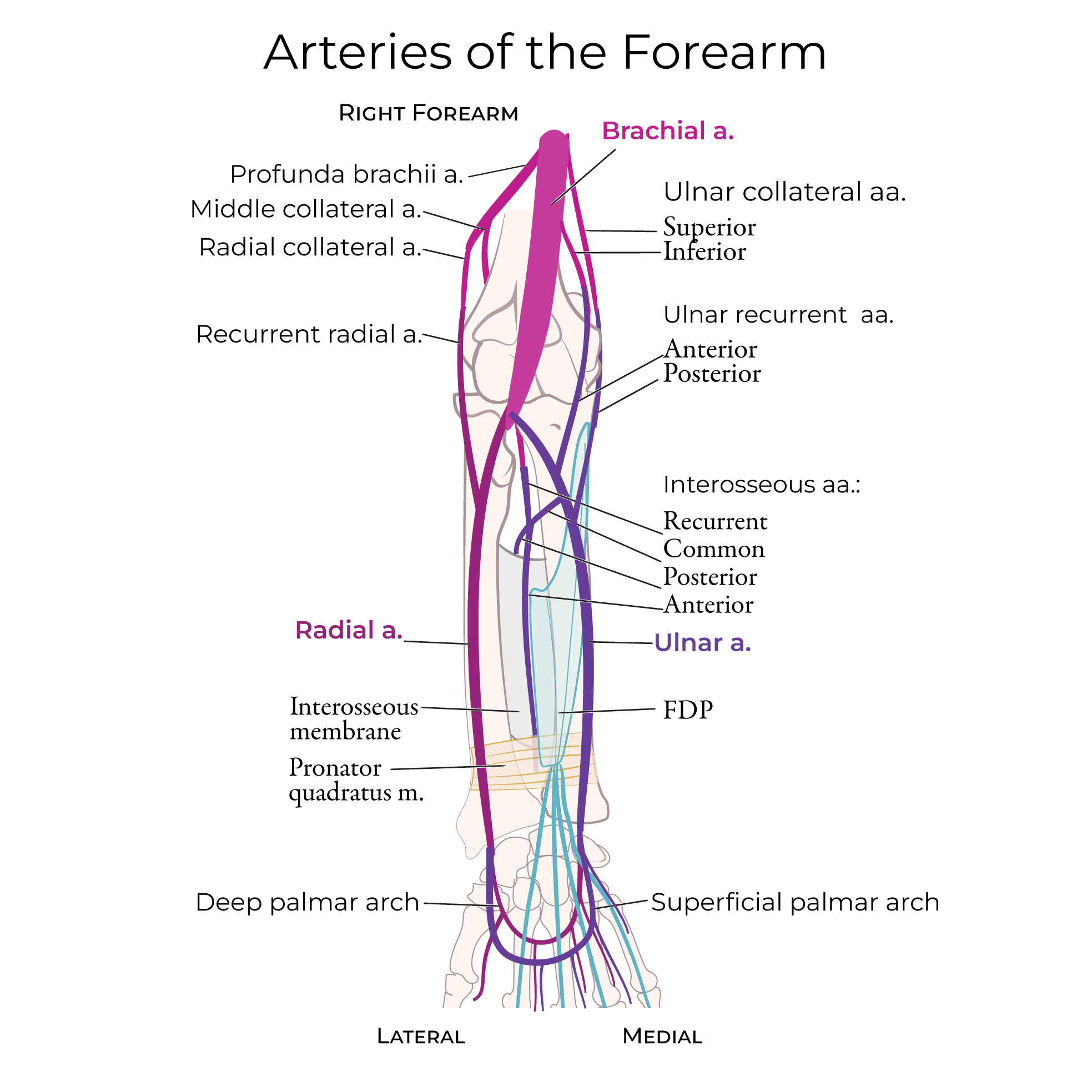
 Blood Supply: An anastomotic network is created by the collateral and recurrent branches of brachial, deep brachial, radial, and ulnar arteries.
Blood Supply: An anastomotic network is created by the collateral and recurrent branches of brachial, deep brachial, radial, and ulnar arteries.
 Innervation: Branches of radial, ulnar, and musculocutaneous nerves.
Innervation: Branches of radial, ulnar, and musculocutaneous nerves.
 The synovial membrane arises from the edges of the articular cartilage of the joints and lines the non-articular boney surface and the inner surface of the fibrous capsule.
The fibrous outer layer of the joint capsule, which attaches to the medial epicondyle and encloses the olecranon, coronoid, and radial fossae. Laterally, the capsule passes around the neck of the radius and coronoid process of ulna.
A pocket of synovial membrane (sacciform recess) protrudes from the inferior free edge of the joint capsule. This protrusion facilitates radial head rotation during pronation and supination.
The fibrous membrane thickens medially and laterally to form the radial ulnar collateral ligaments, which stabilize the joint during forearm flexion and extension. Tendons from brachialis and triceps brachii attach to outside of the joint capsule and help strengthen it.
The external surface of the joint capsule near the radial head is strengthened by the annular ligament of radius; fibers from the annular ligament blend with the radial collateral ligament.
Let's show the collateral ligaments in medial and lateral view.
In medial view, we have a clear look at the humeroulnar joint.
We show the annular ligament of the radius around the head of the radius.
The ulnar collateral ligament has three portions:
The anterior band, which is cord-like; the posterior band, which is fan-like, and the oblique band, which runs under the posterior band. In this view, we can see how the ulnar collateral ligament stabilizes the medial side of the elbow joint.
Next, in lateral view, we'll see the humeroradial joint.
The annular ligament wraps around the head of the radius, the radial collateral ligament connects the humerus and ulna; in this view, we can better see how the fibers from the two ligaments blend.
Supracondylar fracture is a common elbow injury among children, often sustained by falling on an outstretched hand (FOOSH).
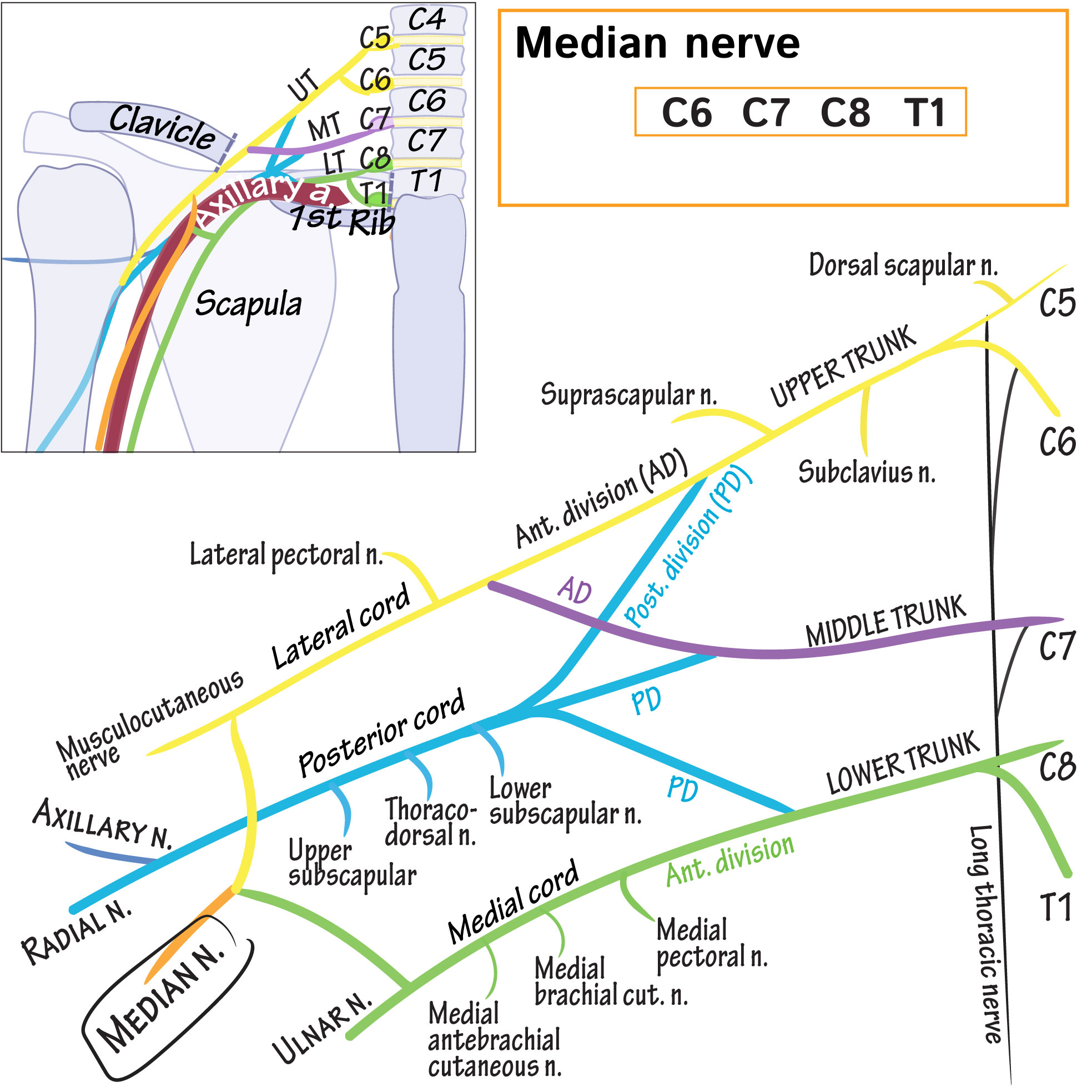
As a result, the brachial artery can be injured, leading to ischemia, and the median nerve can be injured, leading to weak thumb and index finger flexion (when the anterior interosseous branch is involved, patients can't make the "ok" finger sign).
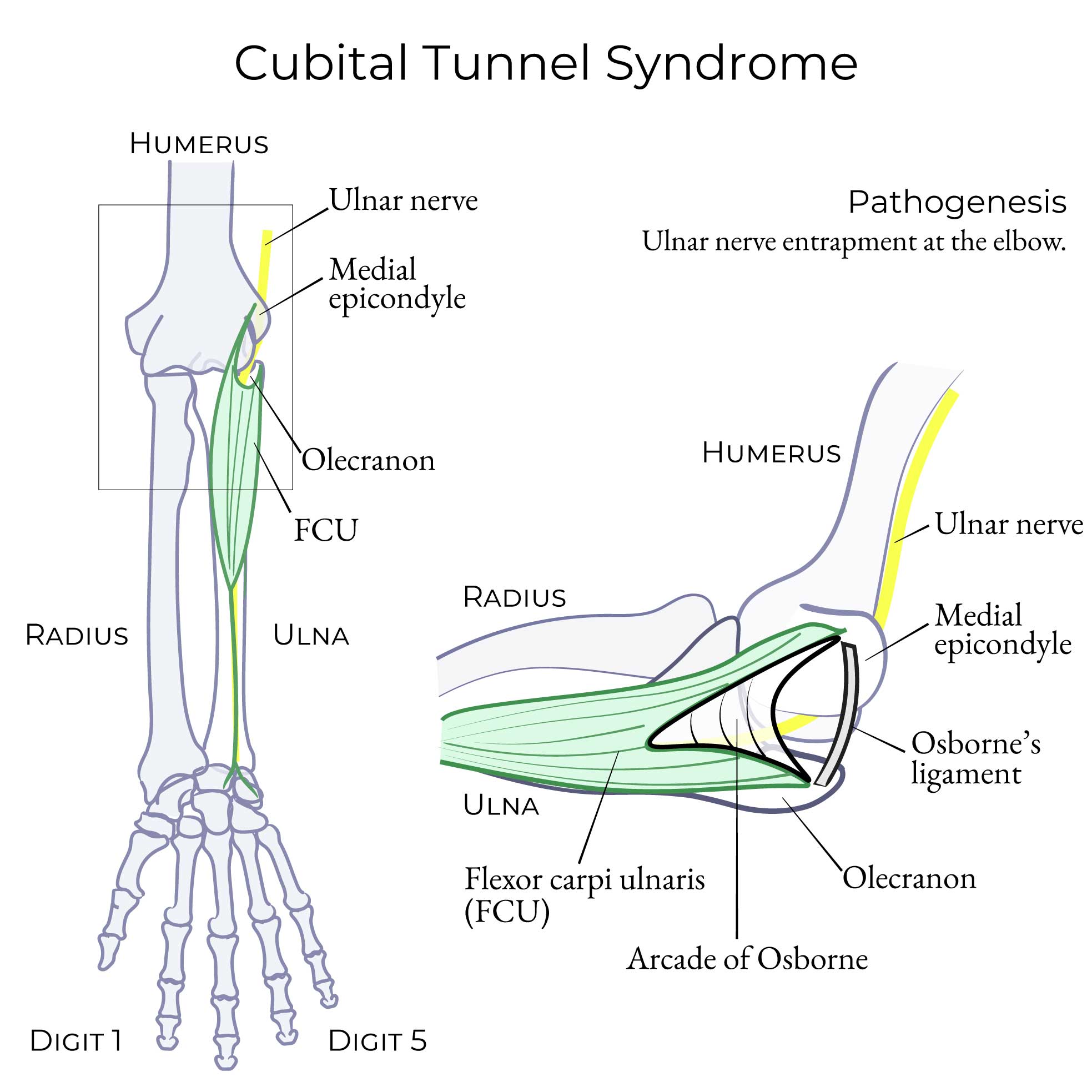
Posterior elbow dislocation can also result from falling on an outstretched hand; posterior elbow dislocation can injure the ulnar nerve, leading to sensory loss in the 4th and 5th digits and weak finger adduction and abduction.
Ulnar collateral ligament injury is often the result of repetitive throwing, and this therefore seen in softball and baseball pitchers. Medial elbow pain and numbness in the 4th and 5th digits is the result of ulnar nerve injury.
The synovial membrane arises from the edges of the articular cartilage of the joints and lines the non-articular boney surface and the inner surface of the fibrous capsule.
The fibrous outer layer of the joint capsule, which attaches to the medial epicondyle and encloses the olecranon, coronoid, and radial fossae. Laterally, the capsule passes around the neck of the radius and coronoid process of ulna.
A pocket of synovial membrane (sacciform recess) protrudes from the inferior free edge of the joint capsule. This protrusion facilitates radial head rotation during pronation and supination.
The fibrous membrane thickens medially and laterally to form the radial ulnar collateral ligaments, which stabilize the joint during forearm flexion and extension. Tendons from brachialis and triceps brachii attach to outside of the joint capsule and help strengthen it.
The external surface of the joint capsule near the radial head is strengthened by the annular ligament of radius; fibers from the annular ligament blend with the radial collateral ligament.
Let's show the collateral ligaments in medial and lateral view.
In medial view, we have a clear look at the humeroulnar joint.
We show the annular ligament of the radius around the head of the radius.
The ulnar collateral ligament has three portions:
The anterior band, which is cord-like; the posterior band, which is fan-like, and the oblique band, which runs under the posterior band. In this view, we can see how the ulnar collateral ligament stabilizes the medial side of the elbow joint.
Next, in lateral view, we'll see the humeroradial joint.
The annular ligament wraps around the head of the radius, the radial collateral ligament connects the humerus and ulna; in this view, we can better see how the fibers from the two ligaments blend.
Supracondylar fracture is a common elbow injury among children, often sustained by falling on an outstretched hand (FOOSH).
As a result, the brachial artery can be injured, leading to ischemia, and the median nerve can be injured, leading to weak thumb and index finger flexion (when the anterior interosseous branch is involved, patients can't make the "ok" finger sign).
Posterior elbow dislocation can also result from falling on an outstretched hand; posterior elbow dislocation can injure the ulnar nerve, leading to sensory loss in the 4th and 5th digits and weak finger adduction and abduction.
Ulnar collateral ligament injury is often the result of repetitive throwing, and this therefore seen in softball and baseball pitchers. Medial elbow pain and numbness in the 4th and 5th digits is the result of ulnar nerve injury.
 From our tutorial on Upper Limb Joint Injuries
From our tutorial on Upper Limb Joint Injuries
Blood Supply: An anastomotic network is created by the collateral and recurrent branches of brachial, deep brachial, radial, and ulnar arteries.
Innervation: Branches of radial, ulnar, and musculocutaneous nerves.
Anterior Elbow
Collateral Ligaments
Clinical Correlations
Elbow
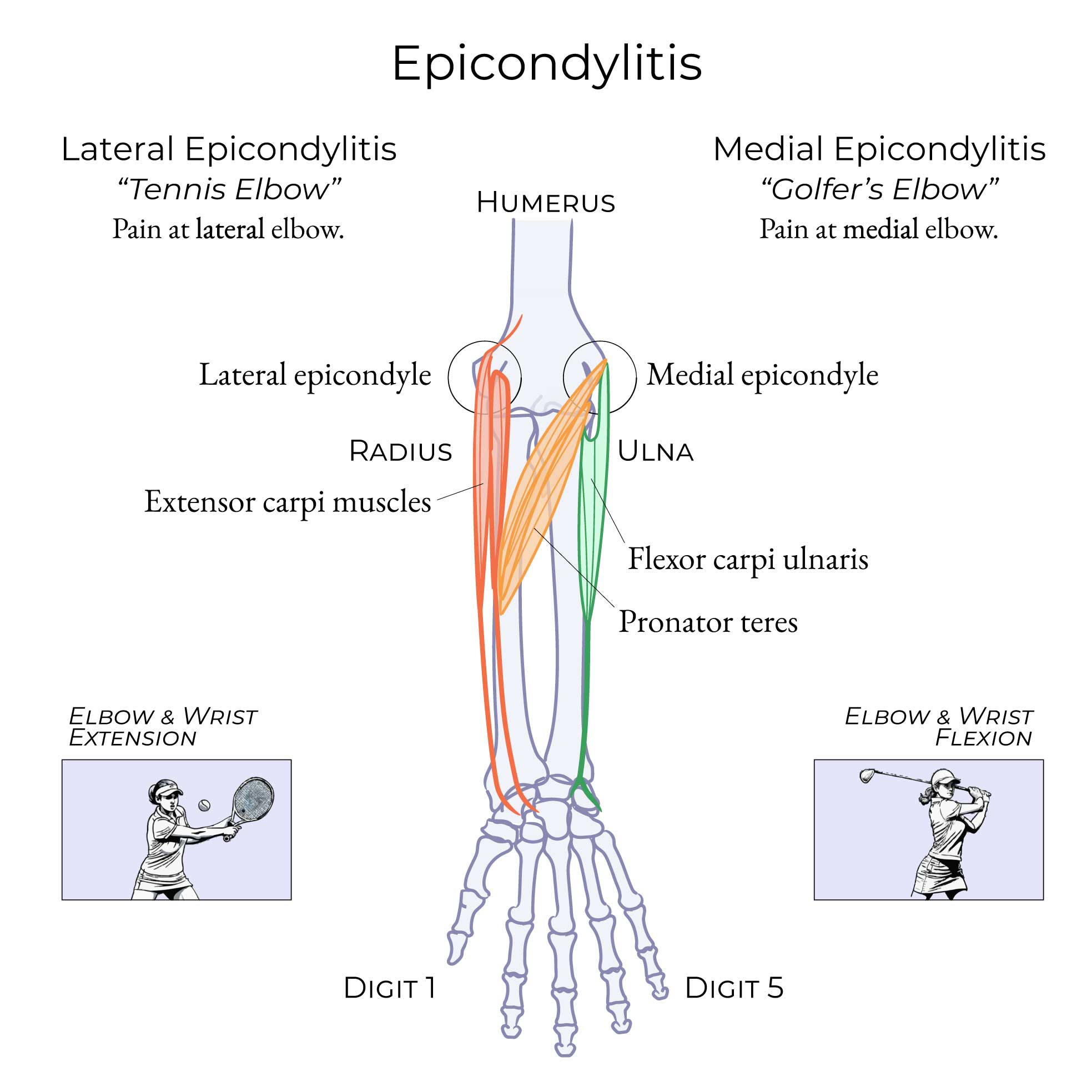
Lateral Epicondylitis (Tennis Elbow)
Mechanism
Occurs from excessive elbow and wrist extension.
- This injury occurs through excessive wrist extension and elbow extension (esp. in forearm supination) with gripping. Think of gripping a tennis racquet and hitting a backhand tennis stroke.
Symptoms
Pain is felt over the lateral epicondyle and radiates into the forearm and wrist.
Key Pathology
Fibrotic tissue invasion and diminished vascularization, called chronic angiofibroblastic tendinosis.
From our tutorial on Upper Limb Joint Injuries
Medial Epicondylitis (Golfer's Elbow)
Occurs from excessive elbow and wrist flexion.
- This injury occurs through excessive wrist and elbow flexion (esp. in forearm pronation) with gripping. Think of over-gripping a golf-club.