

Start your One-Week Free Trial
Already subscribed? Log in »

Congenital Intestinal Defects
Here we will learn some common congenital pathologies of the mid- and hindgut.
 In the absence of rotation, the small intestine lies to the right of the large intestine (thus, this defect is sometimes referred to as “left-sided colon”).
In some cases, the direction of rotation is reversed; rotation occurs clockwise; the duodenum will pass ventral to the transverse colon, instead of dorsal to it.
Mixed rotation occurs when rotation of the cranial and caudal intestinal segments is not coordinated: only the cranial end undergoes the first rotation (90 degrees), and only the caudal end undergoes the second (180 degrees). The cecum lies at the midline, just inferior to the pyloric region of the stomach.
And, because the mesentery is pulled with the intestine as it rotates, mixed rotation can resort in
In the absence of rotation, the small intestine lies to the right of the large intestine (thus, this defect is sometimes referred to as “left-sided colon”).
In some cases, the direction of rotation is reversed; rotation occurs clockwise; the duodenum will pass ventral to the transverse colon, instead of dorsal to it.
Mixed rotation occurs when rotation of the cranial and caudal intestinal segments is not coordinated: only the cranial end undergoes the first rotation (90 degrees), and only the caudal end undergoes the second (180 degrees). The cecum lies at the midline, just inferior to the pyloric region of the stomach.
And, because the mesentery is pulled with the intestine as it rotates, mixed rotation can resort in
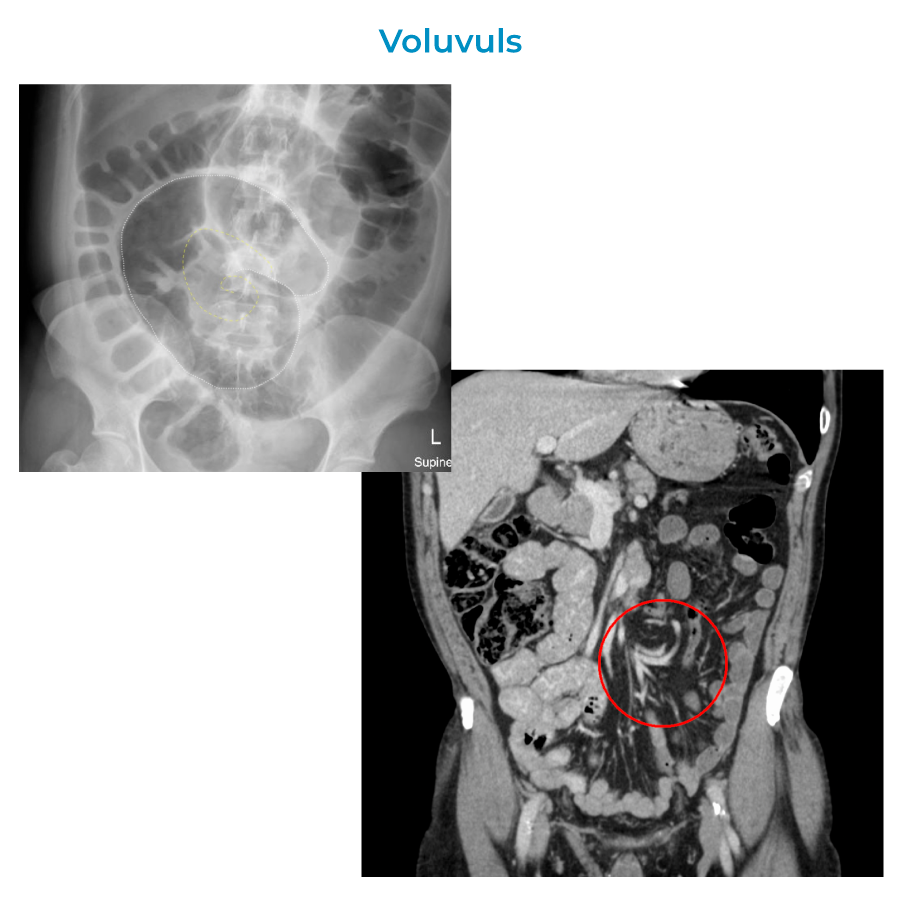 volvulus, aka, torsion, of the mesentery around the superior mesenteric artery. Bands of mesentery (Ladd bands) can constrict and obstruct the digestive tract; the duodenum is particularly susceptible to entrapment by the mesentery of the cecum.
volvulus, aka, torsion, of the mesentery around the superior mesenteric artery. Bands of mesentery (Ladd bands) can constrict and obstruct the digestive tract; the duodenum is particularly susceptible to entrapment by the mesentery of the cecum.
Midgut Congenital Pathologies
Rotational defects of the midgut
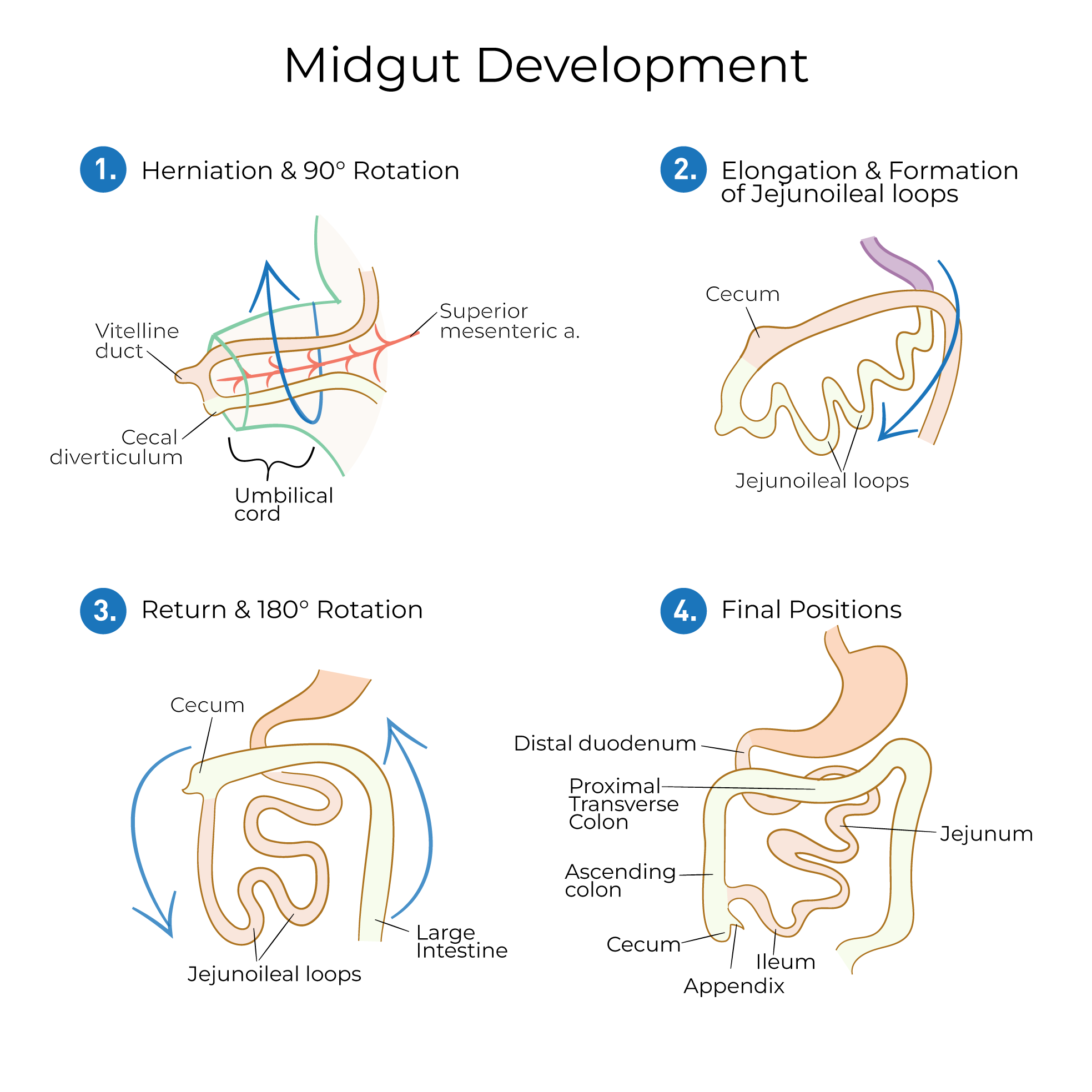
Recall that, typically, the primary intestinal loop undergoes 270 degrees counterclockwise rotation around the superior mesenteric artery as it elongates; in the final position, the large intestine “frames” the small intestine.
In the absence of rotation, the small intestine lies to the right of the large intestine (thus, this defect is sometimes referred to as “left-sided colon”).
In some cases, the direction of rotation is reversed; rotation occurs clockwise; the duodenum will pass ventral to the transverse colon, instead of dorsal to it.
Mixed rotation occurs when rotation of the cranial and caudal intestinal segments is not coordinated: only the cranial end undergoes the first rotation (90 degrees), and only the caudal end undergoes the second (180 degrees). The cecum lies at the midline, just inferior to the pyloric region of the stomach.
And, because the mesentery is pulled with the intestine as it rotates, mixed rotation can resort in
volvulus, aka, torsion, of the mesentery around the superior mesenteric artery. Bands of mesentery (Ladd bands) can constrict and obstruct the digestive tract; the duodenum is particularly susceptible to entrapment by the mesentery of the cecum.
Omphalocele
Omphalocele occurs when the abdominal viscera protrude through the umbilical ring.
The viscera are covered in a thin sac made of the amnion, Wharton’s jelly, and the parietal peritoneum. This sac is susceptible to rupture (not to be confused with gastroschisis, in which the viscera protrude from the anterior body wall but are not covered by a membrane).
Omphalocele is often present in conjunction with other abnormalities and is thought to occur as result of failure to fully retract during midgut rotation, lateral body folding failures, or failure of connective tissues in the abdominal wall.
Meckel’s diverticulum
Meckel’s diverticulum is present when the vitelline duct fails to fully regress. The location and length of the diverticulum are variable, and, in many cases, the anomaly is asymptomatic. However, if the diverticulum contains ectopic gastric tissues, acid secretion can lead to the formation of bleeding ulcers.
Hindgut Congenital Pathologies
Fistulas
A rectourethral fistula occurs when the urinary and digestive tracts are connected; feces can pass into the urine, and urine can pass into the rectum.
Rectovaginal fistulas are characterized by a connection between the vagina and rectum; as a result, rectal contents are directed through the vagina.
Imperforate anus
Presents in various permutations.
Agenesis is characterized by the formation of a blindly ending anorectal canal; the rectum may communicate with the urinary or genital tract via fistula.
Atresia is characterized by obstruction that prevents the anus from opening to the external environment; this may be due to an abnormally thick, persistent anal membrane.