

Start your One-Week Free Trial
Already subscribed? Log in »



Sinus Venosus
Here we will learn about the development of the sinus venosus and its incorporation into adult cardiac features.
Venous blood initially enters the sinus horns of the sinus venosus via paired common cardinal veins.
Between days 24-56, asymmetrical heart and great vessel remodeling directs venous return towards the developing vena cavae and the right side of the heart.
Ultimately, the left sinus horn becomes the coronary sinus (which collects blood from the cardiac veins) and the oblique vein of the left atrium.
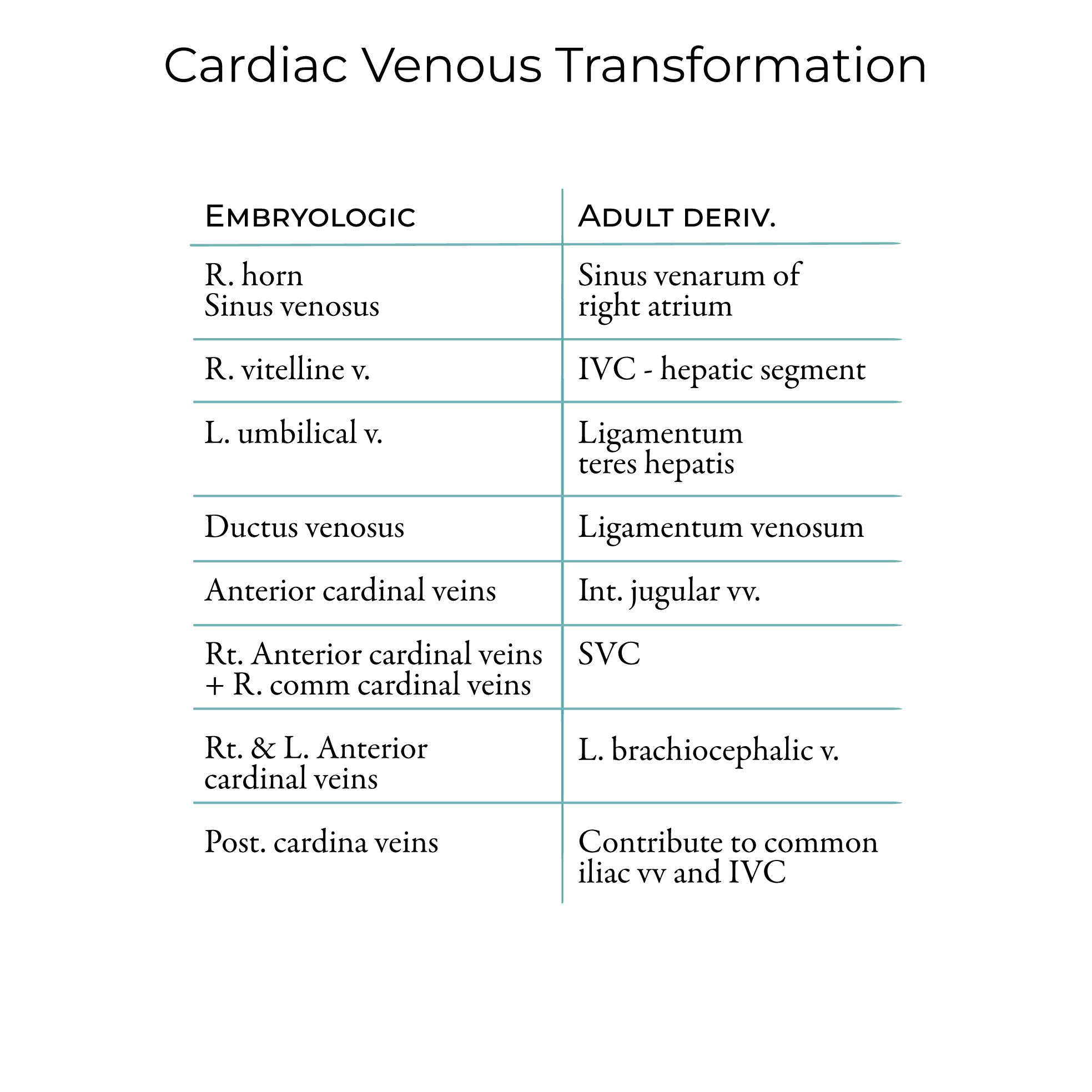
And the right sinus horn is incorporated into the wall of the right atrium (this area of the right atrium is called the sinus venarum).
 Learn more about fetal circulation
Let's begin with a drawing of the primitive heart tube on day 22, prior to heart tube looping.
Venous blood initially enters the caudally located right and left sinus horns of the sinus venosus; from here, it travels cranially through the atrium, ventricle, bulbus cordis, truncus arteriosus, and aortic sac.
By approximately day 24, the venous system remodels to form multiple bilaterally symmetrical venous tracts; many of these tracts will regress.
We show the primitive atria and ventricles in dorsal view.
The outflow tract arises ventrally, and the singular orifice of the pulmonary vein drains into the area of the left atrium.
That the sinus venosus receives blood bilaterally from the sinus horns.
Each sinus horn receives blood from the body via the right and left common cardinal veins, which are formed by the junction of the anterior and posterior cardinal veins.
In addition to the cardinal veins, the right and left umbilical veins deliver oxygenated blood from the placenta to the heart, and the vitelline veins drain the yolk sac.
The common pulmonary vein starts as a midline structure; as we'll see, it shifts to the left and splits to form the four veins of the adult.
Over the next few weeks, venous blood flow shifts to the right.
To show this the shift to the right, we'll draw the heart on day 50.
We re-draw the atria and ventricles; muscular outcroppings of the atria, called auricles, are forming.
The outflow tract has separated into the pulmonary trunk and the ascending aorta. The pulmonary trunk bifurcates to form the pulmonary arteries, which carry blood to the pulmonary circulation, while the aorta carries blood into the systemic circulation.
The original common pulmonary vein has been incorporated into the left atrium, producing four separate pulmonary vein openings.
The sinus venosus and its tributaries as venosus blood return shifts to the right:
The right anterior and common cardinal veins persist, as does the right vitelline vein.
The left vitelline vein and the proximal portions of both umbilical veins have largely regressed. Though not shown here, be aware that the distal left umbilical vein persists and connects to the ductus venosus, allowing oxygenated placental blood to bypass the hepatic sinusoids.
Both posterior cardinal veins largely regress, as does much of the left anterior cardinal vein. Remnants of the posterior cardinal veins contribute to the common iliac veins and to portions of the IVC.
As the left anterior cardinal vein regresses, its small venous branches anastomose with corresponding veins on the right. As we'll see, these anastomoses contribute to formation of the left brachiocephalic vein.
Next, let's see how reorganization of venous return gives rise to the major vessels of the adult form by approximately day 56.
Re-draw the atria, auricles, ventricles, openings of the pulmonary veins, the pulmonary trunk and arteries, and the aorta.
The left sinus horn has become the coronary sinus and oblique vein of the left atrium.
Remnants of the right vitelline vein give rise to the hepatic segment of the inferior vena cava; other segments of the IVC are derived from the subcardinal, supracardinal, and sacrocardinal veins.
The right anterior cardinal vein and right common cardinal veins give rise to the superior vena cava; it receives blood from the right and left brachiocephalic veins.
Recall that the left brachiocephalic vein was formed by anastomoses between the right and left anterior cardinal veins; the right brachiocephalic vein was formed by the right anterior and common cardinal veins and the right horn of the sinus venosus.
Each brachiocephalic vein drains blood from the internal jugular veins, which are also derived from the anterior cardinal veins (the external jugular veins are derived from veins around the head and neck). The brachiocephalic veins also receive blood from the subclavian veins, which drain the upper extremities.
The venous circulation is even more variable than the arteries.
For example, a common variation in the sidedness or number of superior vena cavae results when the left anterior cardinal vein persists.
If the right anterior cardinal/common cardinal venous pathway also persists, a persistent bilateral superior vena cavae is present.
If the right anterior cardinal and common cardinal veins regress and the left veins persist, a left superior vena cava forms.
Learn more about fetal circulation
Let's begin with a drawing of the primitive heart tube on day 22, prior to heart tube looping.
Venous blood initially enters the caudally located right and left sinus horns of the sinus venosus; from here, it travels cranially through the atrium, ventricle, bulbus cordis, truncus arteriosus, and aortic sac.
By approximately day 24, the venous system remodels to form multiple bilaterally symmetrical venous tracts; many of these tracts will regress.
We show the primitive atria and ventricles in dorsal view.
The outflow tract arises ventrally, and the singular orifice of the pulmonary vein drains into the area of the left atrium.
That the sinus venosus receives blood bilaterally from the sinus horns.
Each sinus horn receives blood from the body via the right and left common cardinal veins, which are formed by the junction of the anterior and posterior cardinal veins.
In addition to the cardinal veins, the right and left umbilical veins deliver oxygenated blood from the placenta to the heart, and the vitelline veins drain the yolk sac.
The common pulmonary vein starts as a midline structure; as we'll see, it shifts to the left and splits to form the four veins of the adult.
Over the next few weeks, venous blood flow shifts to the right.
To show this the shift to the right, we'll draw the heart on day 50.
We re-draw the atria and ventricles; muscular outcroppings of the atria, called auricles, are forming.
The outflow tract has separated into the pulmonary trunk and the ascending aorta. The pulmonary trunk bifurcates to form the pulmonary arteries, which carry blood to the pulmonary circulation, while the aorta carries blood into the systemic circulation.
The original common pulmonary vein has been incorporated into the left atrium, producing four separate pulmonary vein openings.
The sinus venosus and its tributaries as venosus blood return shifts to the right:
The right anterior and common cardinal veins persist, as does the right vitelline vein.
The left vitelline vein and the proximal portions of both umbilical veins have largely regressed. Though not shown here, be aware that the distal left umbilical vein persists and connects to the ductus venosus, allowing oxygenated placental blood to bypass the hepatic sinusoids.
Both posterior cardinal veins largely regress, as does much of the left anterior cardinal vein. Remnants of the posterior cardinal veins contribute to the common iliac veins and to portions of the IVC.
As the left anterior cardinal vein regresses, its small venous branches anastomose with corresponding veins on the right. As we'll see, these anastomoses contribute to formation of the left brachiocephalic vein.
Next, let's see how reorganization of venous return gives rise to the major vessels of the adult form by approximately day 56.
Re-draw the atria, auricles, ventricles, openings of the pulmonary veins, the pulmonary trunk and arteries, and the aorta.
The left sinus horn has become the coronary sinus and oblique vein of the left atrium.
Remnants of the right vitelline vein give rise to the hepatic segment of the inferior vena cava; other segments of the IVC are derived from the subcardinal, supracardinal, and sacrocardinal veins.
The right anterior cardinal vein and right common cardinal veins give rise to the superior vena cava; it receives blood from the right and left brachiocephalic veins.
Recall that the left brachiocephalic vein was formed by anastomoses between the right and left anterior cardinal veins; the right brachiocephalic vein was formed by the right anterior and common cardinal veins and the right horn of the sinus venosus.
Each brachiocephalic vein drains blood from the internal jugular veins, which are also derived from the anterior cardinal veins (the external jugular veins are derived from veins around the head and neck). The brachiocephalic veins also receive blood from the subclavian veins, which drain the upper extremities.
The venous circulation is even more variable than the arteries.
For example, a common variation in the sidedness or number of superior vena cavae results when the left anterior cardinal vein persists.
If the right anterior cardinal/common cardinal venous pathway also persists, a persistent bilateral superior vena cavae is present.
If the right anterior cardinal and common cardinal veins regress and the left veins persist, a left superior vena cava forms.
Learn more about fetal circulation
Day 22
Day 24
Day 50
Day 56
Clinical Correlations