

Start your One-Week Free Trial
Already subscribed? Log in »



Heart Tube Formation
Here we will learn about formation of the primitive heart tube, which is the result of fusion of bilateral endocardial tubes.
Progenitor heart cells arise from epiblast cells that ingress through the primitive streak on approximately day 16.
These cells migrate through the splanchnic layer of the lateral plate mesoderm and form blood islands in the cardiogenic region.
Blood islands give rise to angiogenic cords that become paired endocardial tubes.
A single endocardial primitive heart tube forms when lateral embryonic folding facilitates fusion of the paired tubes.
On approximately days 19 and 20, myocardial progenitor cells surround the heart tube; they start to form the myocardium and secrete cardiac jelly. By days 21-22, functional contractions begin.
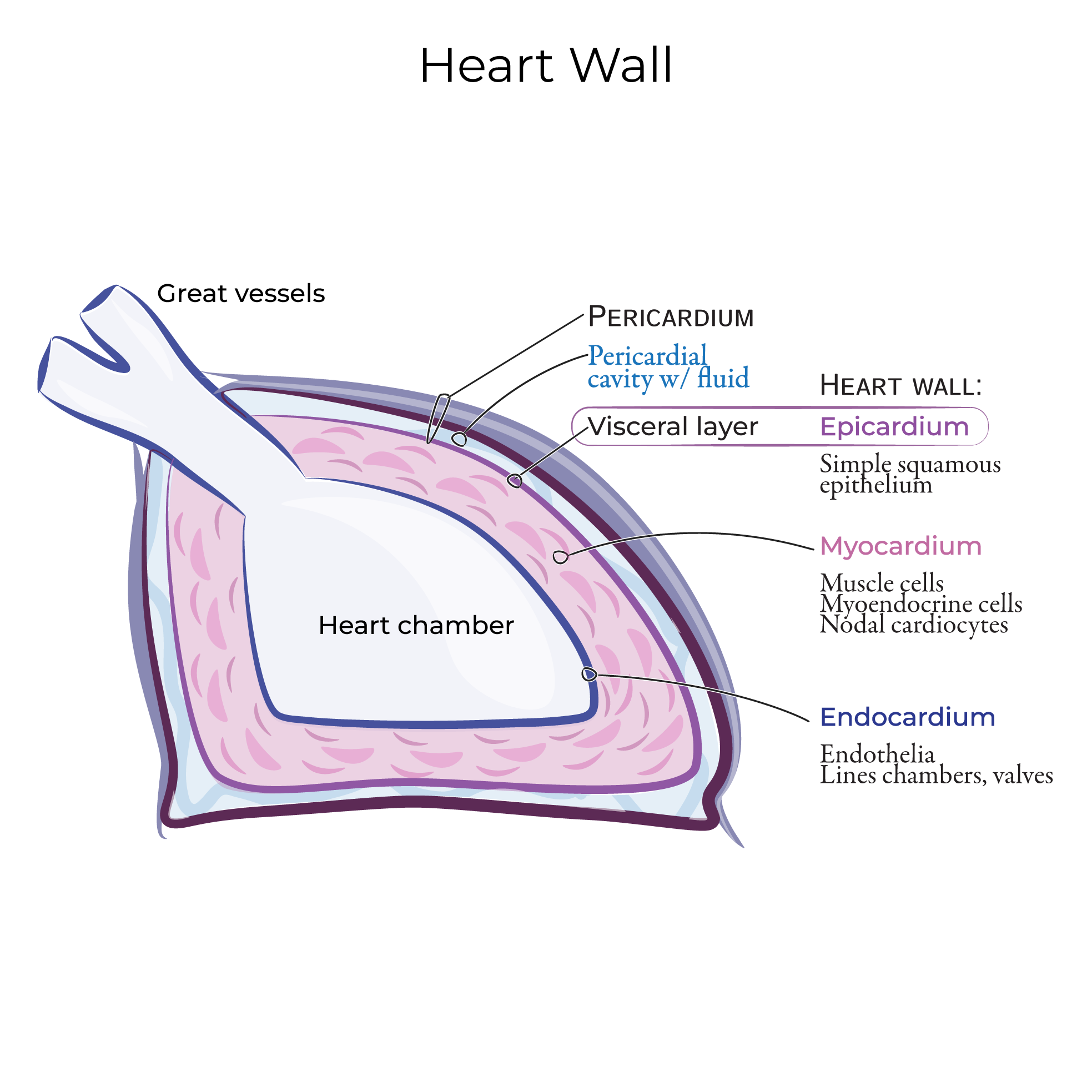
Soon, the heart tube will comprise 3 layers: an inner endocardium, muscular myocardium, and outer epicardium.
 In this tutorial, we’ll focus on the origins and formation of the endocardium and myocardium but be aware that the epicardium arises from the proepicardial organ. The proepicardial organ arises from a mass of mesodermal cells near the septum transversum and migrates over the myocardium.
Cardia bifida is characterized by the formation of two heart tubes as a result of defects in lateral folding; the two tubes cannot effectively pump blood, so the condition is fatal.
Dextrocardia and situs inversus are characterized by abnormal right-left patterning that occurs when left-right patterning is disrupted. In patients with dextrocardia, the heart is on the right side of the thorax instead of the left; situs inversus is the condition in which the rest of the visceral organs are also reversed. Although these conditions are often asymptomatic, they can be associated with severe heart defects.
Excessive retinoic acid exposure during cardiac development in weeks 3-4 can lead to major septal and conotruncal defects; be aware that high levels of retinoids, such as isotretinoin, are found in some prescription oral medications that treat acne.
In this tutorial, we’ll focus on the origins and formation of the endocardium and myocardium but be aware that the epicardium arises from the proepicardial organ. The proepicardial organ arises from a mass of mesodermal cells near the septum transversum and migrates over the myocardium.
Cardia bifida is characterized by the formation of two heart tubes as a result of defects in lateral folding; the two tubes cannot effectively pump blood, so the condition is fatal.
Dextrocardia and situs inversus are characterized by abnormal right-left patterning that occurs when left-right patterning is disrupted. In patients with dextrocardia, the heart is on the right side of the thorax instead of the left; situs inversus is the condition in which the rest of the visceral organs are also reversed. Although these conditions are often asymptomatic, they can be associated with severe heart defects.
Excessive retinoic acid exposure during cardiac development in weeks 3-4 can lead to major septal and conotruncal defects; be aware that high levels of retinoids, such as isotretinoin, are found in some prescription oral medications that treat acne.
Overview
In this tutorial, we’ll focus on the origins and formation of the endocardium and myocardium but be aware that the epicardium arises from the proepicardial organ. The proepicardial organ arises from a mass of mesodermal cells near the septum transversum and migrates over the myocardium.
~Day 18
Dorsal view
We show the mesoderm, then the overlying epiblast; we draw it only on the caudal end of the embryo so we can see the mesoderm at the cranial end.
In the ectoderm, we show the primitive streak; at its cranial 1/3rd, we show the cardiac progenitor cells.
The cardiac progenitor cells ingress through the streak and migrate cranially and laterally through the mesoderm to form the cardiac crescent; these cells comprise the 1st heart field.
The 1st heart field ultimately gives rise to parts of the left and right atria, the left ventricle, and a portion of the right ventricle.
The second heart field lies ventral to the pharynx in the splanchnic mesoderm.
The second heart field gives rise to the rest of the right ventricle, and the outflow tracts (including the bulbus cordis and the truncus arteriosus), and contributes to formation of the atria.
After establishing the first heart field, the cells of the cardiac crescent differentiate into cardiac myoblasts and blood islands. The blood islands undergo vasculogenesis to form early blood cells and vessels; in the splanchnic mesoderm, blood islands give rise to angioblastic cords that become paired endocardial tubes.
Transverse view
First, we draw the amniotic cavity, which is lined by ectoderm, and the yolk sac, which is lined by endoderm.
Then, we show the mesoderm; the mesoderm overlying the amniotic cavity comprises the parietal, aka, somatic mesoderm, whereas the mesoderm overlying the yolk sac comprises splanchnic, aka, visceral mesoderm.
We label the intra-embryonic cavity, which will eventually be divided to form the pleural, pericardial, and peritoneal cavities.
Now, within the splanchnic mesoderm, we show myocardial precursors.
Within the splanchnic mesoderm, we indicate the bilateral endocardial tubes, which are derived from the angioblastic cords that we mentioned a moment ago.
Dorsally, we show the paired aortae, which form from angioblastic cords that lie close to the midline.
Over the next few days, lateral embryonic folding facilitates fusion of the endocardial tubes, while cephalic folding brings the heart and pericardial cavity into the thorax.
~Day 22
Transverse view
The amnion (aka, amniotic membrane) envelops the embryo.
We show the surface ectoderm, and that the neural plate has folded to create the neural tube, and that cells at the edge of the neural tube have differentiated to become neural crest cells.
Show the paired dorsal aortae and the foregut.
The primitive heart tube formed when the paired endocardial tubes fused at midline. It comprises an inner endocardial tube and an outer myocardium; between these two layers, show the cardiac jelly, which is produced by the myocardium. Cardiac jelly is an extracellular matrix that provides structure for the developing heart walls.
Indicate that the bilateral parietal mesoderm fused and now contributes to the body wall, and the splanchnic mesoderm covers the ventral surface of the foregut.
Label the dorsal mesocardium, which secures the primitive heart tube to the parietal pericardium; as we learn elsewhere, the degeneration of the dorsal mesocardium gives rise to the transverse sinus.
Then, label the pericardial cavity, which is the space surrounding the primitive heart tube.
Heart tube in coronal section
Outline the tube, which comprises the endocardium, myocardium, and cardiac jelly.
The epicardium arises from the proepicardial organ, and is here beginning to cover the surface of the heart; it will later contribute to the connective tissue and smooth muscle of the coronary vessels.
Now, show the sections of the heart tube in the direction of blood flow, from caudal to cranial:
Right and left horns of the sinus venosus
Atrium
Ventricle
Bulbus cordis
Truncus arteriosus
And, finally, the aortic sac; as we’ll discuss elsewhere, the aortic sac gives rise to the aortic arches.
Clinical Correlations