

Start your One-Week Free Trial
Already subscribed? Log in »

Cleavage & Implantation
Overview
Cleavage
Key Steps:
Zygote, single cell, produced by fusion of the male and female gametes in fertilization; surrounded by zona pellucida, which is the acellular protective coat.
After a single round of mitosis, the zygote gives rise to two cells, aka, blastomeres.
By the four-cell stage, the blastomeres are loosely organized, with incomplete contact between the cells.
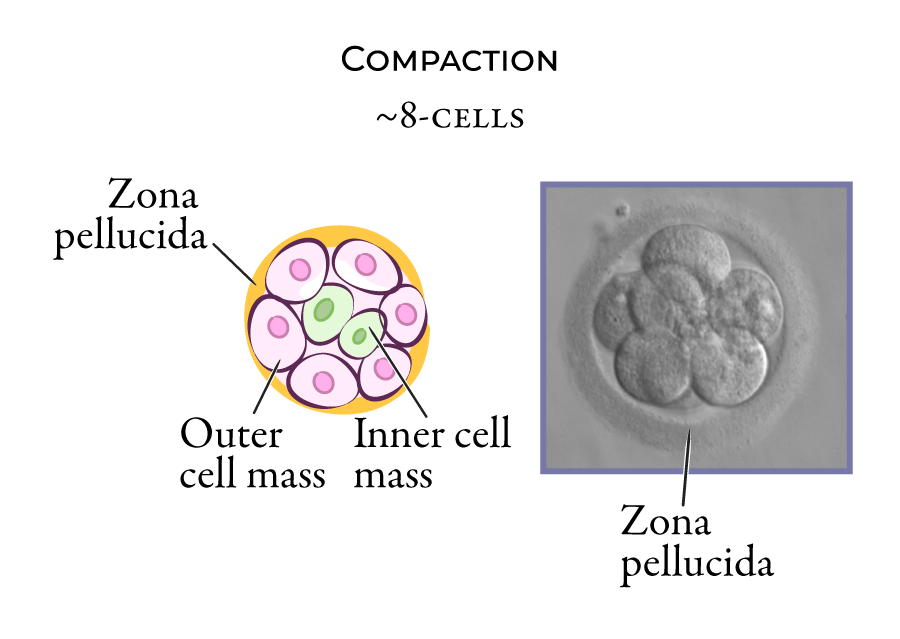
This changes at the 8-cell stage, when compaction reorganizes the cells and forms:
- An inner cell mass, which is held together by tight junctions.
- An outer cell mass, which is covered by the zona pellucida.
 In the next stage the morula comprises approximately 16 cells. Sodium-potassium pumps pull water into the morula cell mass; as a result, cavitation occurs
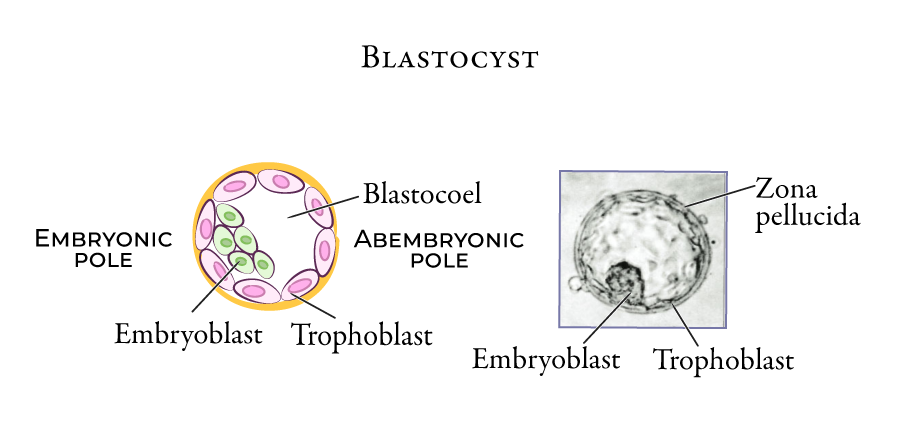
Morula gives rise to the blastocyst, with a blastocyst cavity (blastocoel)
In the blastocyst, the zona pellucida surrounds two cell populations:
Outer cell population is now called the trophoblast.
Inner cell mass, which has become concentrated to one side, is now called the embryoblast.
In the next stage the morula comprises approximately 16 cells. Sodium-potassium pumps pull water into the morula cell mass; as a result, cavitation occurs
Morula gives rise to the blastocyst, with a blastocyst cavity (blastocoel)
In the blastocyst, the zona pellucida surrounds two cell populations:
Outer cell population is now called the trophoblast.
Inner cell mass, which has become concentrated to one side, is now called the embryoblast.
 As we learn elsewhere, the trophoblast plays an essential role in implantation and formation of the placenta, and the embryoblast gives rise to the tissues of the embryo proper.
Cavitation establishes embryonic polarity:
As we learn elsewhere, the trophoblast plays an essential role in implantation and formation of the placenta, and the embryoblast gives rise to the tissues of the embryo proper.
Cavitation establishes embryonic polarity:
- Embryonic pole at the side of the embryoblast.
- Abembryonic pole at the opposite side.
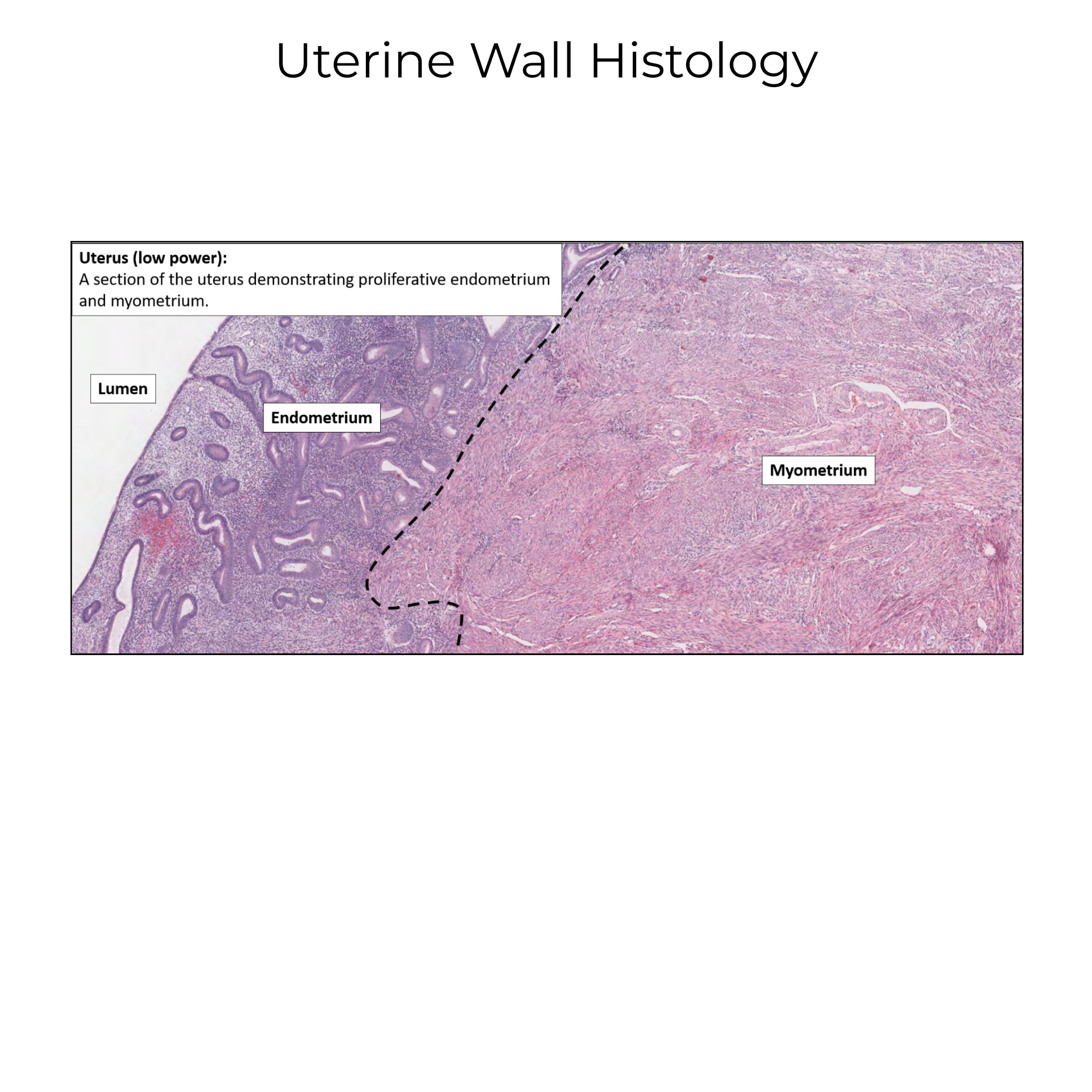
Implantation
Implantation window:
The days of the cycle when the endometrium is receptive to implantation.
The window typically begins 6-8 days after ovulation, and lasts approximately 4 days.
Prior to the implantation window, the endometrial lining is thinner and has not yet released pro-embryo secretions; after this window, the endometrial lining prepares for shedding during menstruation.
Iimplantation
1. Pre-implantation events, which include "hatching" of the blastocyst from the zona pellucida.
2. Blastocyst apposition to the uterine wall.
3. Early adhesion to uterine epithelia.
4. Uterine stroma – embryo contact, which ultimately connects the maternal vascular supply to the embryo.
Step 1
In response to ovarian hormones, the stroma has undergone decidualization, and is edematous, vascularized, and rich in mucus and glycogen. Thus, the endometrium is ready to house and nourish an embryo.
The blastocyst emerges from the zona pellucida (aka, it "hatches"), and can interact directly with the maternal environment.
The embryo releases substances that prevent its rejection. One of these substances, human chorionic growth hormone (hCG), preserves the corpus luteum within the ovary; recall that the corpus luteum produces progesterone, which is necessary for maintenance of the endometrial lining, and, therefore, the survival of the embryo.
Thus, many early pregnancy tests rely on the presence of hCG to determine pregnancy status.
Step 2
Apposition involves alignment of the embryonic pole to the uterine wall, to which it loosely attaches.
The blastocyst rolls over the surface of the uterus (some texts specify that it is the inner cell mass that "rolls" within the trophoblast).
Proper alignment relies on signaling between the epithelia and embryo: pinopods, aka, uterodomes, on the uterine wall interact with microvilli on the blastocyst and establish a loose connection.
Step 3
Receptor-ligand signaling facilitates initial adhesion of the blastocyst to the epithelia. More specifically, chemokine reactions appear to play a significant role.
Step 4
The trophoblast transforms as the embryo begins to sink into the endometrial stroma.
The trophoblast gives rise to the cytotrophoblast and synctiotrophoblast, which we show in shades of green and blue.
The syncytiotrophoblast produces proteolytic enzymes and other substances that interact with the uterine stroma to facilitate implantation.
The endometrial stroma plays an active role in this process, as recent research indicates that stromal cells are highly motile, and move around the embryo to envelop it.
As part of this process, extensive vascular remodeling of the stroma allows maternal oxygen and nutrients to reach the developing embryo. Elsewhere, we'll learn how embryonic and maternal tissues transform to produce the multi-functional placenta.
Clinical Correlations
Implantation Failure
More than half of all conceptions are spontaneously aborted. In many cases, this is because of embryonic chromosomal abnormalities: blastocysts that fail to produce hCG, for example, are rejected by the maternal environment. In this way, the endometrium acts as a "bio-sensor" that detects when an embryo is of poor quality and rejects it as a way to prevent investment in offspring that are unlikely to survive.
In other cases, the endometrium is unreceptive because of increased inflammation, hormonal abnormalities, or other health issues.
Ectopic Pregnancy
Ectopic pregnancies occur when implantation occurs outside of the uterus; it occurs in 1-2% of all pregnancies.
Ectopic pregnancies most often happen in the uterine tube when blastocyst transport is impaired, but they can also occur within the abdominopelvic cavity.
An ectopic pregnancy poses a serious danger to the woman, particularly because its rupture leads to internal bleeding.